Department of Neurosurgery, Heidelberg University, Im Neuenheimer Feld 400, Heidelberg, 69120, Germany.
Department of Neurosurgery, Heidelberg University Hospital, Im Neuenheimer Feld 400, Heidelberg, 69120, Germany.
Pituitary. 2023 Aug;26(4):451-460. doi: 10.1007/s11102-023-01333-4. Epub 2023 Jun 30.
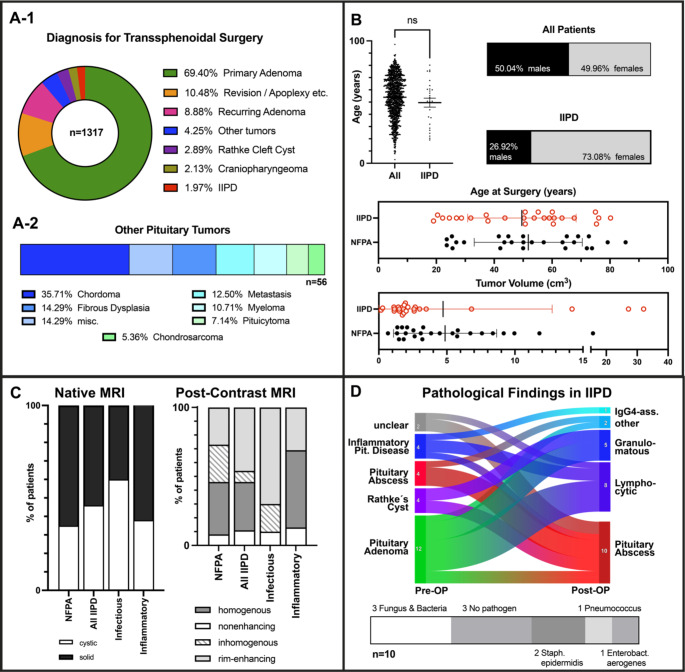
Inflammatory and infectious diseases of the pituitary gland (IIPD) are rare lesions often misdiagnosed preoperatively. Immediate surgery is indicated especially in cases of neurological impairment. However, (chronic) inflammatory processes can mimic other pituitary tumors, such as adenomas, and data on the preoperative diagnostic criteria for IIPD are sparse.
We retrospectively reviewed medical records of 1317 patients who underwent transsphenoidal surgery at our institution between March 2003 and January 2023. A total of 26 cases of histologically confirmed IIPD were identified. Patient records, laboratory parameters, and postoperative course were analyzed and compared with an age, sex, and tumor volume-matched control group of nonfunctioning pituitary adenomas.
Pathology confirmed septic infection in ten cases, most commonly caused by bacteria (3/10) and fungi (2/10). In the aseptic group, lymphocytic hypophysitis (8/26) and granulomatous inflammation (3/26) were most frequently observed. Patients with IIPD commonly presented with endocrine and/or neurological dysfunction. No surgical mortality occurred. Preoperative radiographic findings (cystic/solid tumor mass, contrast enhancement) did not significantly differ between IIPD and adenomas. At follow-up, 13 patients required permanent hormone substitution.
In conclusion, correct preoperative diagnosis of IIPD remains challenging, as neither radiographic findings nor preoperative laboratory workup unequivocally identify these lesions. Surgical treatment facilitates decompression of supra- and parasellar structures. Furthermore, this low-morbidity procedure enables the identification of pathogens or inflammatory diseases requiring targeted medical treatment, which is crucial for these patients. Establishing a correct diagnosis through surgery and histopathological confirmation thus remains of utmost importance.
垂体炎性和感染性疾病(IIPD)是罕见的病变,常被误诊。特别是在有神经功能障碍的情况下,需要立即手术。然而,(慢性)炎症过程可能会模仿其他垂体肿瘤,如腺瘤,并且关于 IIPD 的术前诊断标准的数据很少。
我们回顾性分析了 2003 年 3 月至 2023 年 1 月期间在我们机构接受经蝶窦手术的 1317 例患者的病历。共确定了 26 例经组织学证实的 IIPD。分析患者的病历、实验室参数和术后病程,并与非功能性垂体腺瘤的年龄、性别和肿瘤体积匹配的对照组进行比较。
病理证实十例为感染性疾病,最常见的病原体为细菌(3/10)和真菌(2/10)。在无菌性组中,最常观察到淋巴细胞性垂体炎(8/26)和肉芽肿性炎症(3/26)。IIPD 患者常出现内分泌和/或神经功能障碍。无手术死亡。术前影像学检查(囊性/实性肿瘤、对比增强)在 IIPD 和腺瘤之间无显著差异。随访时,13 例患者需要永久性激素替代治疗。
总之,正确诊断 IIPD 仍然具有挑战性,因为影像学发现和术前实验室检查均不能明确识别这些病变。手术治疗有助于缓解鞍上和鞍旁结构的压迫。此外,这种低并发症手术可以识别需要靶向治疗的病原体或炎症性疾病,这对这些患者至关重要。因此,通过手术和组织病理学确认建立正确的诊断仍然至关重要。