Center for Brain Circuit Therapeutics, Departments of Neurology, Psychiatry and Radiology, Brigham and Women's Hospital, Boston, Massachusetts.
Harvard Medical School, Harvard University, Boston, Massachusetts.
JAMA Neurol. 2023 Sep 1;80(9):891-902. doi: 10.1001/jamaneurol.2023.1988.
It remains unclear why lesions in some locations cause epilepsy while others do not. Identifying the brain regions or networks associated with epilepsy by mapping these lesions could inform prognosis and guide interventions.
To assess whether lesion locations associated with epilepsy map to specific brain regions and networks.
DESIGN, SETTING, AND PARTICIPANTS: This case-control study used lesion location and lesion network mapping to identify the brain regions and networks associated with epilepsy in a discovery data set of patients with poststroke epilepsy and control patients with stroke. Patients with stroke lesions and epilepsy (n = 76) or no epilepsy (n = 625) were included. Generalizability to other lesion types was assessed using 4 independent cohorts as validation data sets. The total numbers of patients across all datasets (both discovery and validation datasets) were 347 with epilepsy and 1126 without. Therapeutic relevance was assessed using deep brain stimulation sites that improve seizure control. Data were analyzed from September 2018 through December 2022. All shared patient data were analyzed and included; no patients were excluded.
Epilepsy or no epilepsy.
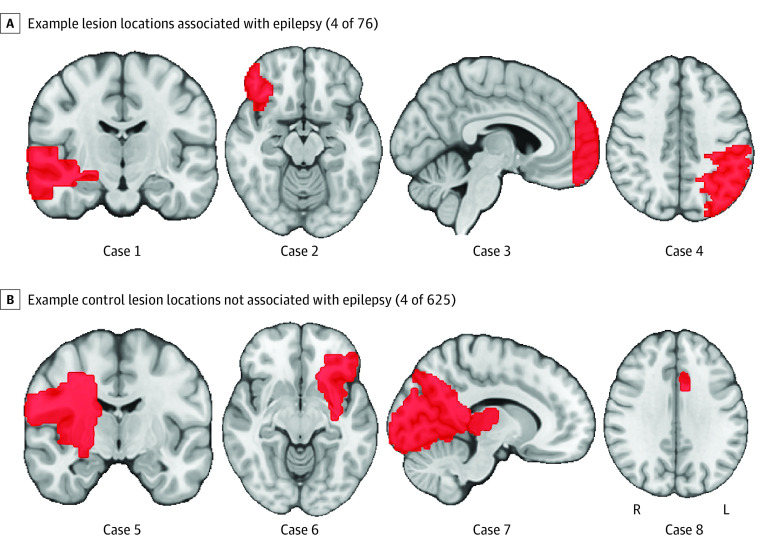
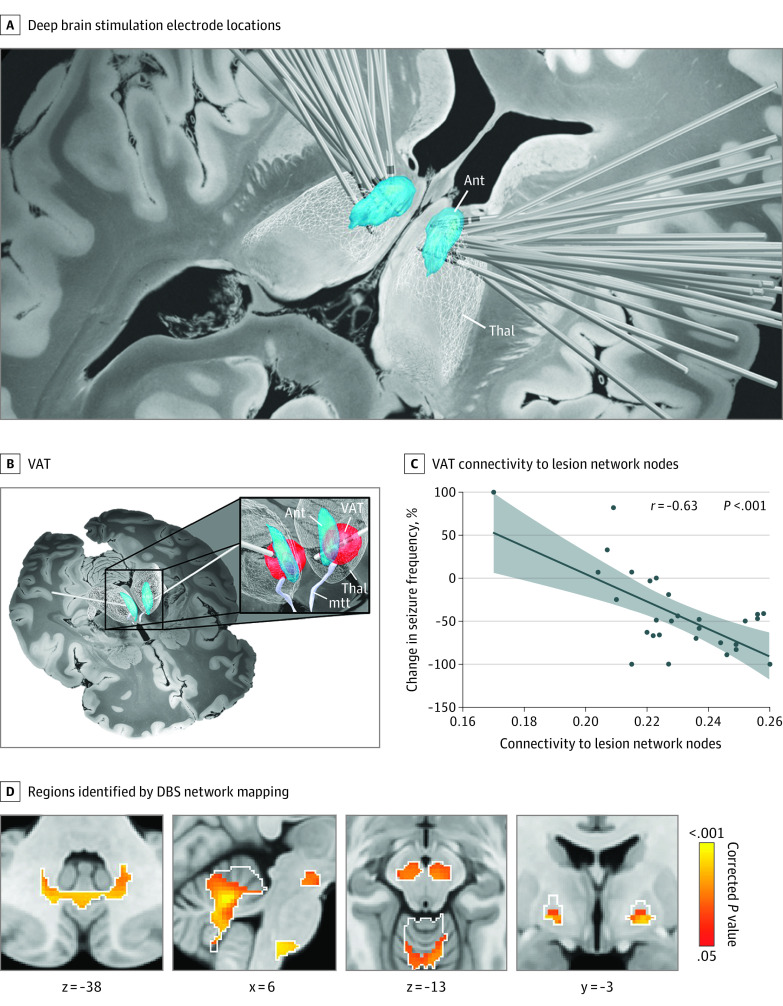
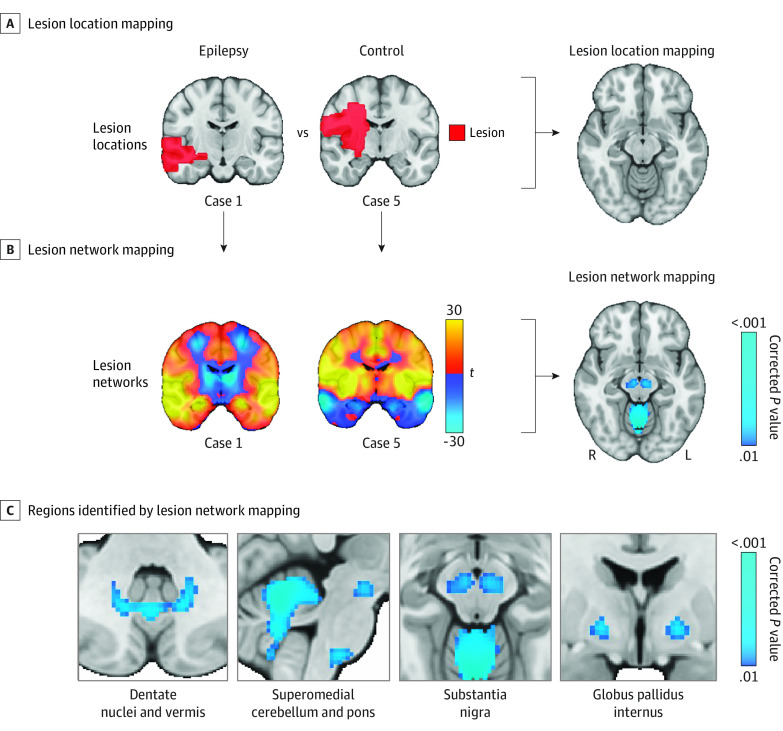
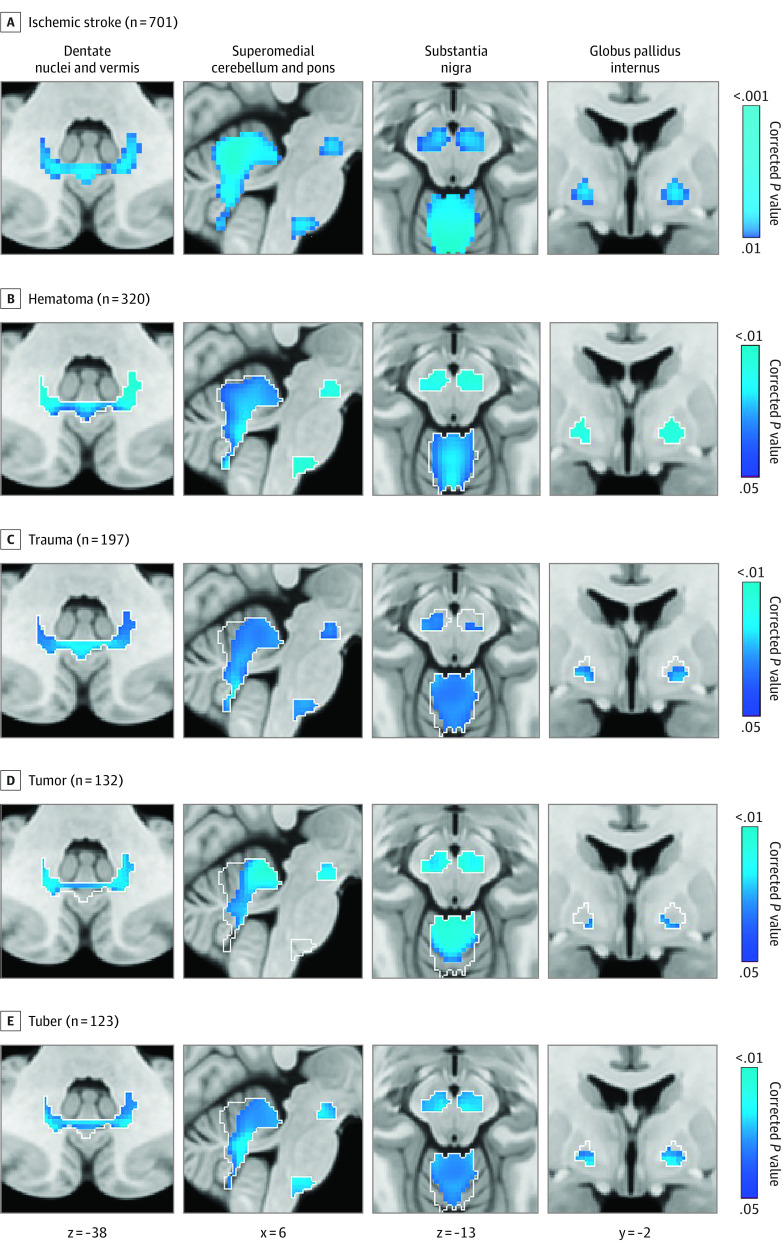
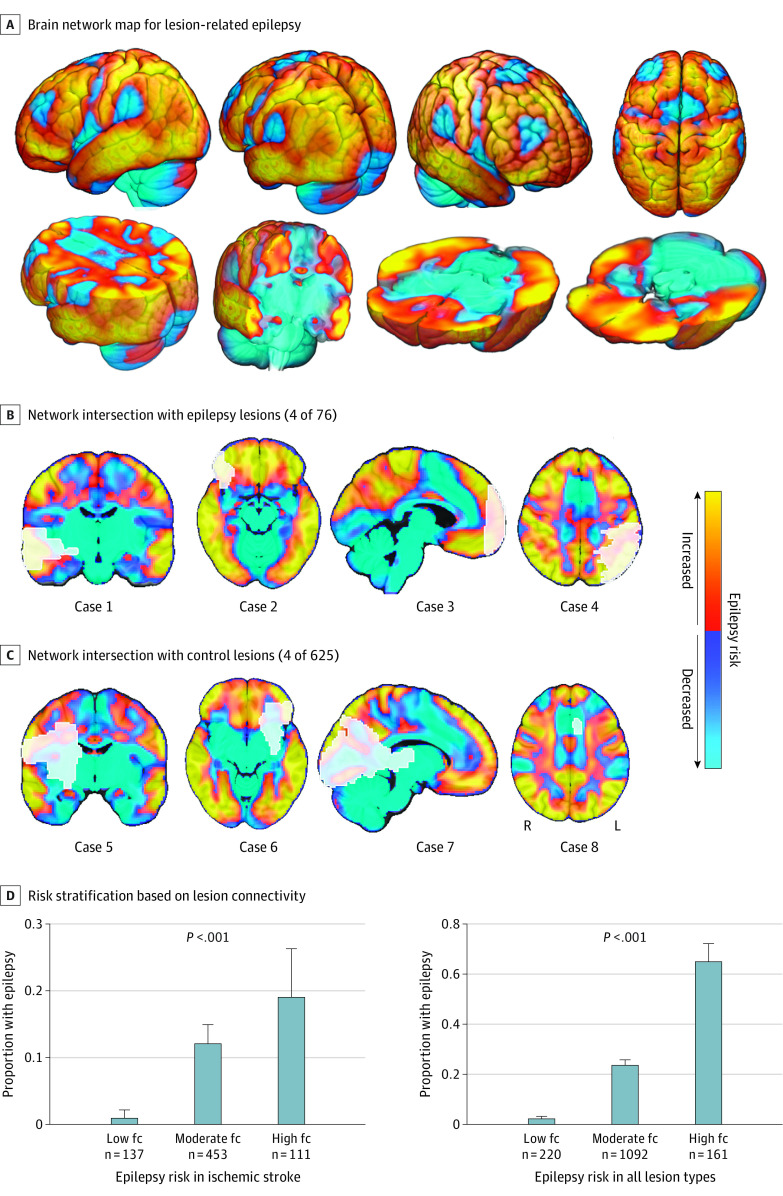
Lesion locations from 76 patients with poststroke epilepsy (39 [51%] male; mean [SD] age, 61.0 [14.6] years; mean [SD] follow-up, 6.7 [2.0] years) and 625 control patients with stroke (366 [59%] male; mean [SD] age, 62.0 [14.1] years; follow-up range, 3-12 months) were included in the discovery data set. Lesions associated with epilepsy occurred in multiple heterogenous locations spanning different lobes and vascular territories. However, these same lesion locations were part of a specific brain network defined by functional connectivity to the basal ganglia and cerebellum. Findings were validated in 4 independent cohorts including 772 patients with brain lesions (271 [35%] with epilepsy; 515 [67%] male; median [IQR] age, 60 [50-70] years; follow-up range, 3-35 years). Lesion connectivity to this brain network was associated with increased risk of epilepsy after stroke (odds ratio [OR], 2.82; 95% CI, 2.02-4.10; P < .001) and across different lesion types (OR, 2.85; 95% CI, 2.23-3.69; P < .001). Deep brain stimulation site connectivity to this same network was associated with improved seizure control (r, 0.63; P < .001) in 30 patients with drug-resistant epilepsy (21 [70%] male; median [IQR] age, 39 [32-46] years; median [IQR] follow-up, 24 [16-30] months).
The findings in this study indicate that lesion-related epilepsy mapped to a human brain network, which could help identify patients at risk of epilepsy after a brain lesion and guide brain stimulation therapies.
某些部位的病变导致癫痫,而其他部位的病变则不导致癫痫,其原因仍不清楚。通过对这些病变进行定位,确定与癫痫相关的大脑区域或网络,可以为预后提供信息,并指导干预措施。
评估与癫痫相关的病变部位是否与特定的大脑区域和网络相关联。
设计、地点和参与者:这项病例对照研究使用病变部位和病变网络映射,在一个包括中风后癫痫患者和无癫痫中风对照患者的发现数据集,确定与癫痫相关的大脑区域和网络。纳入了有中风病变和癫痫(n=76)或无癫痫(n=625)的患者。使用 4 个独立的队列作为验证数据集,评估了对其他病变类型的推广能力。所有数据集(发现和验证数据集)中癫痫患者的总人数为 347 人,无癫痫患者的总人数为 1126 人。使用改善癫痫控制的深部脑刺激部位评估治疗相关性。数据于 2018 年 9 月至 2022 年 12 月进行分析。所有共享的患者数据都进行了分析和纳入,没有排除任何患者。
癫痫或无癫痫。
纳入了 76 例中风后癫痫患者(39 例[51%]为男性;平均[标准差]年龄为 61.0[14.6]岁;平均[标准差]随访时间为 6.7[2.0]年)和 625 例中风对照患者(366 例[59%]为男性;平均[标准差]年龄为 62.0[14.1]岁;随访时间范围为 3-12 个月)的病变位置在发现数据集中进行了分析。与癫痫相关的病变发生在多个不同的叶和血管区域的异质位置。然而,这些相同的病变位置是由与基底节和小脑的功能连接定义的特定大脑网络的一部分。在包括 772 例脑病变患者的 4 个独立队列中验证了这些发现(271 例[35%]有癫痫;515 例[67%]为男性;中位数[四分位数间距]年龄为 60[50-70]岁;随访时间范围为 3-35 年)。该脑网络与中风后癫痫风险增加相关(优势比[OR],2.82;95%置信区间[CI],2.02-4.10;P<0.001),且与不同病变类型相关(OR,2.85;95% CI,2.23-3.69;P<0.001)。该网络与深部脑刺激部位的连接与 30 例药物难治性癫痫患者(21 例[70%]为男性;中位数[四分位数间距]年龄为 39[32-46]岁;中位数[四分位数间距]随访时间为 24[16-30]个月)的癫痫控制改善相关(r,0.63;P<0.001)。
这项研究的结果表明,与病变相关的癫痫与人类大脑网络有关,这有助于识别脑损伤后癫痫风险患者,并指导脑刺激治疗。