Subdivision of Endocrinology and Metabolism, Health Screening and Promotion Center, Asan Medical Center, Seoul, Korea.
Subdivision of Gastroenterology and Hepatology, Health Screening and Promotion Center, Asan Medical Center, Seoul, Korea.
Clin Mol Hepatol. 2023 Oct;29(4):987-1001. doi: 10.3350/cmh.2023.0035. Epub 2023 Jul 5.
BACKGROUND/AIMS: To investigate whether non-alcoholic fatty liver disease (NAFLD) in individuals without generalized obesity is associated with visceral fat obesity (VFO), sarcopenia, and/or myosteatosis.
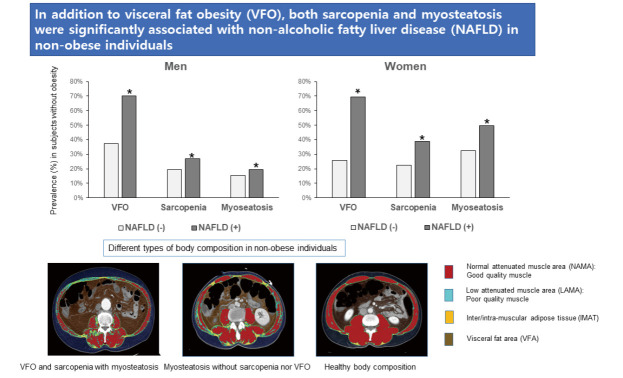
This cross-sectional analysis included 14,400 individuals (7,470 men) who underwent abdominal computed tomography scans during routine health examinations. The total abdominal muscle area (TAMA) and skeletal muscle area (SMA) at the 3rd lumbar vertebral level were measured. The SMA was divided into the normal attenuation muscle area (NAMA) and low attenuation muscle area, and the NAMA/TAMA index was calculated. VFO was defined by visceral to subcutaneous fat ratio, sarcopenia by body mass index-adjusted SMA, and myosteatosis by the NAMA/TAMA index. NAFLD was diagnosed with ultrasonography.
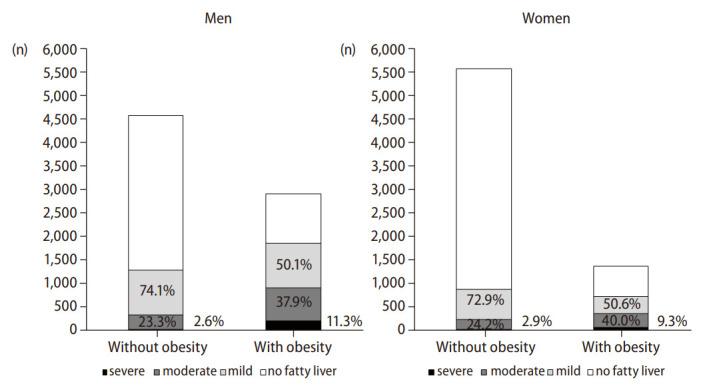
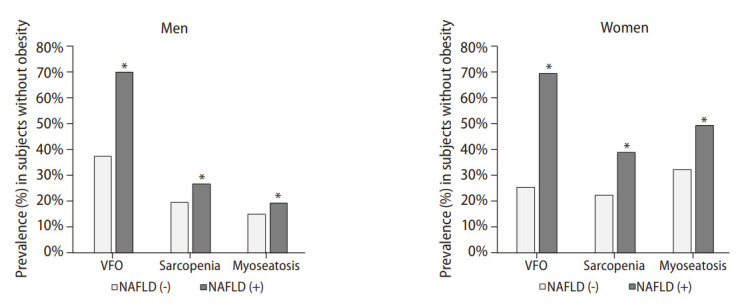
Of the 14,400 individuals, 4,748 (33.0%) had NAFLD, and the prevalence of NAFLD among non-obese individuals was 21.4%. In regression analysis, both sarcopenia (men: odds ratio [OR] 1.41, 95% confidence interval [CI] 1.19-1.67, P<0.001; women: OR=1.59, 95% CI 1.40-1.90, P<0.001) and myosteatosis (men: OR=1.24, 95% CI 1.02-1.50, P=0,028; women: OR=1.23, 95% CI 1.04-1.46, P=0.017) were significantly associated with non-obese NAFLD after considering for VFO and other various risk factors, whereas VFO (men: OR=3.97, 95% CI 3.43-4.59 [adjusted for sarcopenia], OR 3.98, 95% CI 3.44-4.60 [adjusted for myosteatosis]; women: OR=5.42, 95% CI 4.53-6.42 [adjusted for sarcopenia], OR=5.33, 95% CI 4.51-6.31 [adjusted for myosteatosis]; all P<0.001) was strongly associated with non-obese NAFLD after adjustment with various known risk factors.
In addition to VFO, sarcopenia and/or myosteatosis were significantly associated with non-obese NAFLD.
背景/目的:研究非肥胖个体的非酒精性脂肪肝(NAFLD)是否与内脏脂肪肥胖(VFO)、肌少症和/或肌脂肪变性有关。
本横断面分析纳入了 14400 名(男 7470 名)在常规健康检查中接受腹部计算机断层扫描的个体。测量第 3 腰椎水平的总腹部肌肉面积(TAMA)和骨骼肌面积(SMA)。将 SMA 分为正常衰减肌肉面积(NAMA)和低衰减肌肉面积,并计算 NAMA/TAMA 指数。VFO 定义为内脏与皮下脂肪比,肌少症定义为体重指数校正后的 SMA,肌脂肪变性定义为 NAMA/TAMA 指数。NAFLD 通过超声诊断。
在 14400 名个体中,4748 名(33.0%)患有 NAFLD,非肥胖个体中 NAFLD 的患病率为 21.4%。在回归分析中,肌少症(男性:比值比[OR]1.41,95%置信区间[CI]1.19-1.67,P<0.001;女性:OR=1.59,95%CI 1.40-1.90,P<0.001)和肌脂肪变性(男性:OR=1.24,95%CI 1.02-1.50,P=0.028;女性:OR=1.23,95%CI 1.04-1.46,P=0.017)与非肥胖性 NAFLD 显著相关,在考虑 VFO 和其他各种危险因素后,而 VFO(男性:OR=3.97,95%CI 3.43-4.59[校正肌少症],OR 3.98,95%CI 3.44-4.60[校正肌脂肪变性];女性:OR=5.42,95%CI 4.53-6.42[校正肌少症],OR=5.33,95%CI 4.51-6.31[校正肌脂肪变性];均 P<0.001)与非肥胖性 NAFLD 密切相关,在调整各种已知危险因素后。
除 VFO 外,肌少症和/或肌脂肪变性与非肥胖性 NAFLD 显著相关。