Rashmi Priyanka, Sigdel Tara K, Rychkov Dmitry, Damm Izabella, Da Silva Andrea Alice, Vincenti Flavio, Lourenco Andre L, Craik Charles S, Reiser Jochen, Sarwal Minnie M
Department of Surgery, University of California San Francisco, San Francisco, CA, USA.
Department of Immunology, Laboratory of Autoimmunity and Immunoregulation, Fluminense Federal University, Niteroi, Brazil.
Ann Transl Med. 2023 Jun 30;11(9):315. doi: 10.21037/atm-22-3670. Epub 2023 May 4.
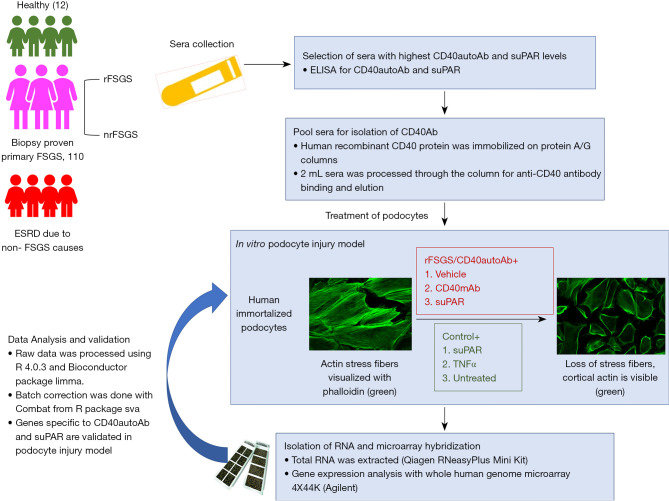
Focal segmental glomerulosclerosis (FSGS) is frequently associated with heavy proteinuria and progressive renal failure requiring dialysis or kidney transplantation. However, primary FSGS also has a ~40% risk of recurrence of disease in the transplanted kidney (rFSGS). Multiple circulating factors have been identified to contribute to the pathogenesis of primary and rFSGS including soluble urokinase-type plasminogen activator receptor (suPAR) and patient-derived CD40 autoantibody (CD40autoAb). However, the downstream effector pathways specific to individual factors require further study. The tumor necrosis factor, TNF pathway activation by one or more circulating factors present in the sera of patients with FSGS has been supported by multiple studies.
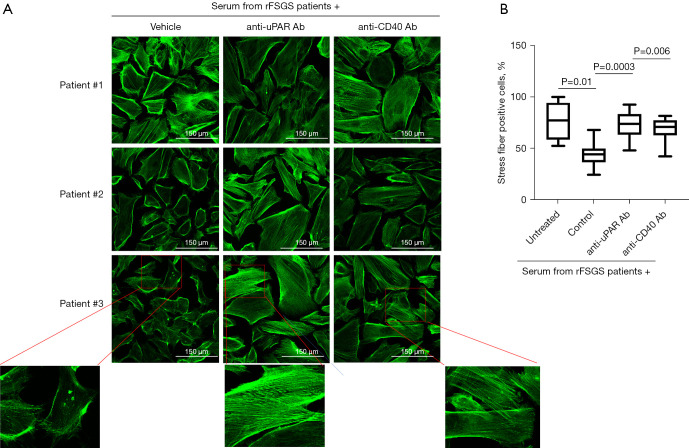
A human model was used to study podocyte injury measured as the loss of actin stress fibers. Anti-CD40 autoantibody was isolated from FSGS patients (recurrent and non-recurrent) and control patients with ESRD due to non-FSGS related causes. Two novel human antibodies-anti-uPAR (2G10) and anti-CD40 antibody (Bristol Meyer Squibb, 986090) were tested for their ability to rescue podocyte injury. Podocytes treated with patient derived antibody were transcriptionally profiled using whole human genome microarray.
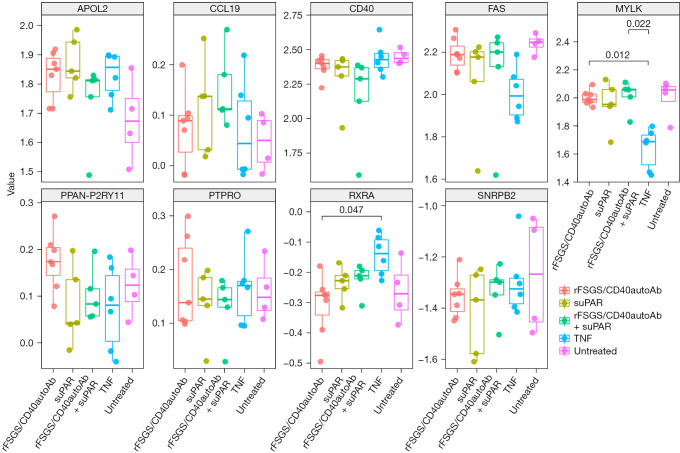
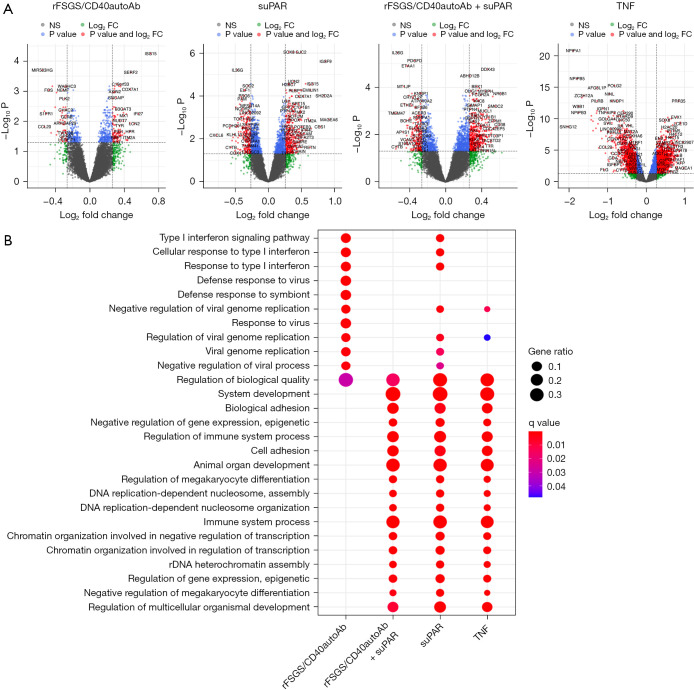
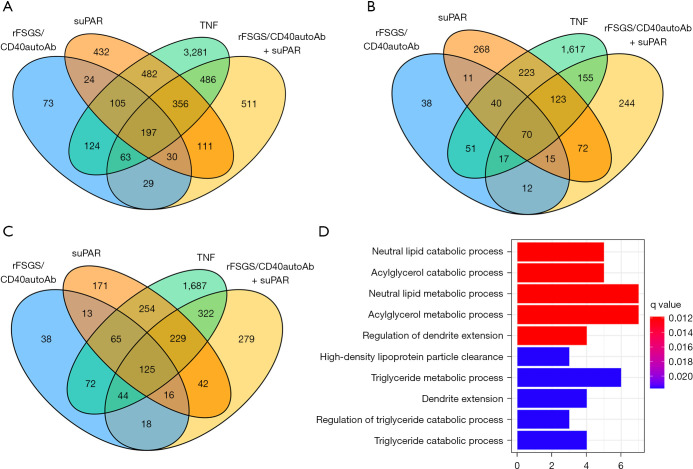
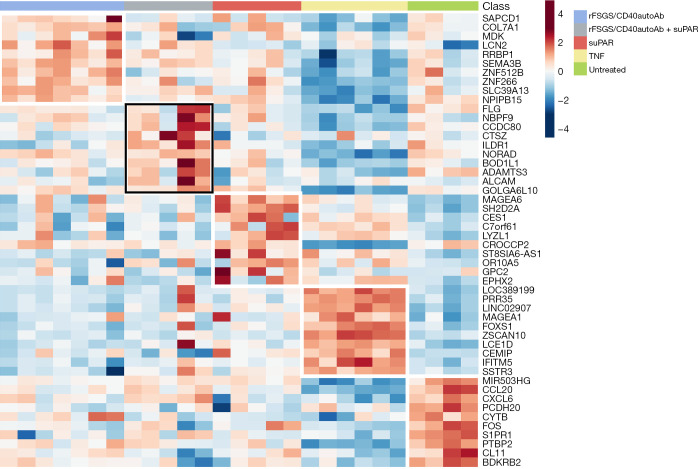
Here we show that podocyte injury caused by sera from FSGS patients is mediated by CD40 and suPAR and can be blocked by human anti-uPAR and anti-CD40 antibodies. Transcriptomic studies to compare the molecules and pathways activated in response to CD40 autoantibody from rFSGS patients (rFSGS/CD40autoAb) and suPAR, identified unique inflammatory pathways associated with FSGS injury.
We identified several novel and previously described genes associated with FSGS progression. Targeted blockade of suPAR and CD40 pathways with novel human antibodies showed inhibition of podocyte injury in FSGS.
局灶节段性肾小球硬化(FSGS)常伴有大量蛋白尿和进展性肾衰竭,需要透析或肾移植。然而,原发性FSGS在移植肾中也有~40%的疾病复发风险(rFSGS)。已确定多种循环因子参与原发性和rFSGS的发病机制,包括可溶性尿激酶型纤溶酶原激活物受体(suPAR)和患者来源的CD40自身抗体(CD40autoAb)。然而,特定因子的下游效应途径需要进一步研究。多项研究支持FSGS患者血清中一种或多种循环因子激活肿瘤坏死因子(TNF)途径。
使用人模型研究以肌动蛋白应力纤维丧失衡量的足细胞损伤。从FSGS患者(复发和非复发)以及因非FSGS相关原因导致的终末期肾病(ESRD)对照患者中分离抗CD40自身抗体。测试两种新型人源抗体——抗uPAR(2G10)和抗CD40抗体(百时美施贵宝,986090)挽救足细胞损伤的能力。用患者来源抗体处理的足细胞使用全人类基因组微阵列进行转录谱分析。
我们在此表明,FSGS患者血清引起的足细胞损伤由CD40和suPAR介导,可被人抗uPAR和抗CD40抗体阻断。转录组学研究比较了rFSGS患者的CD40自身抗体(rFSGS/CD40autoAb)和suPAR激活的分子和途径,确定了与FSGS损伤相关的独特炎症途径。
我们鉴定了几个与FSGS进展相关的新基因和先前描述的基因。用新型人源抗体靶向阻断suPAR和CD40途径可抑制FSGS中的足细胞损伤。