Stovall Stephanie Lee, Kaplan Jennifer A, Law Joanna K, Flum David R, Simianu Vlad V
Department of Surgery, Virginia Mason Franciscan Health, Seattle, WA 98101, United States.
Department of Gastroenterology, Virginia Mason Franciscan Health, Seattle, WA 98101, United States.
World J Gastrointest Surg. 2023 Jun 27;15(6):1007-1019. doi: 10.4240/wjgs.v15.i6.1007.
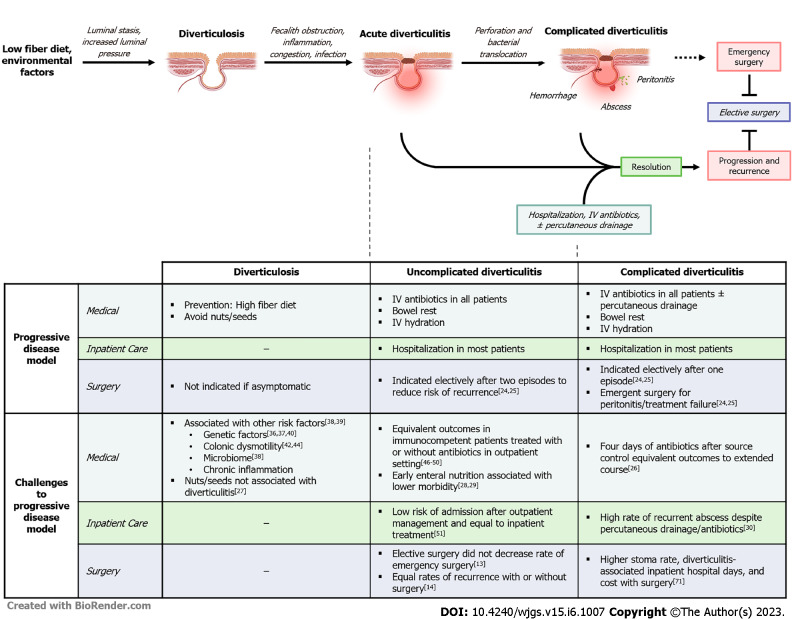
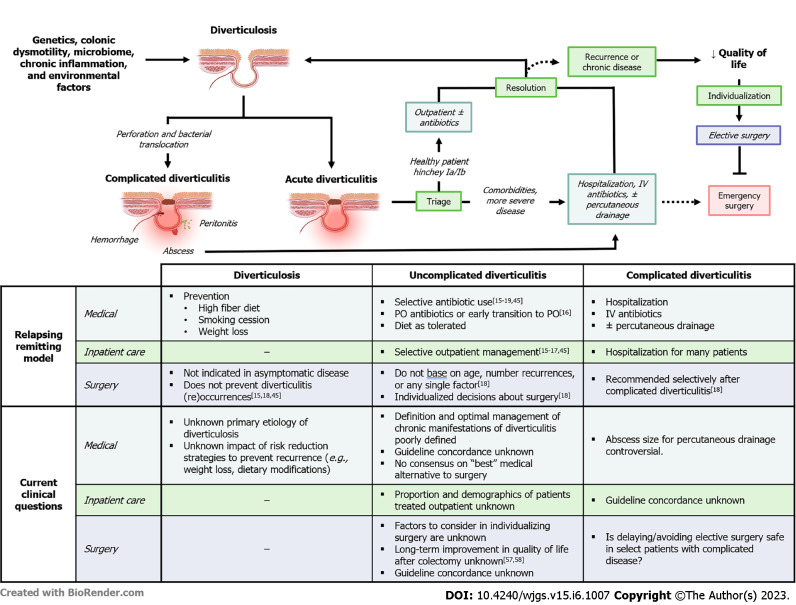
The disease burden of diverticulitis is high across inpatient and outpatient settings, and the prevalence of diverticulitis has increased. Historically, patients with acute diverticulitis were admitted routinely for intravenous antibiotics and many had urgent surgery with colostomy or elective surgery after only a few episodes. Several recent studies have challenged the standards of how acute and recurrent diverticulitis are managed, and many clinical practice guidelines (CPGs) have pivoted to recommend outpatient management and individualized decisions about surgery. Yet the rates of diverticulitis hospitalizations and operations are increasing in the United States, suggesting there is a disconnect from or delay in adoption of CPGs across the spectrum of diverticular disease. In this review, we propose approaching diverticulitis care from a population level to understand the gaps between contemporary studies and real-world practice and suggest strategies to implement and improve future care.
憩室炎在住院和门诊环境中的疾病负担都很高,且憩室炎的患病率有所上升。从历史上看,急性憩室炎患者通常会因静脉使用抗生素而住院,许多患者在仅发作几次后就进行了紧急造口手术或择期手术。最近的几项研究对急性和复发性憩室炎的管理标准提出了挑战,许多临床实践指南(CPG)已转向推荐门诊管理以及关于手术的个体化决策。然而,美国憩室炎的住院率和手术率正在上升,这表明在整个憩室病范围内,CPG的采用存在脱节或延迟。在本综述中,我们建议从人群层面来处理憩室炎的护理问题,以了解当代研究与现实世界实践之间的差距,并提出实施和改善未来护理的策略。