Department of Anesthesiology-L.E.I.C.A., Amsterdam University Medical Centers, Location AMC, Cardiovascular Science, Meibergdreef 11, 1105 AZ Amsterdam, The Netherlands.
Department of Anesthesiology, Kerckhoff-Clinic-Center for Heart, Lung, Vascular and Rheumatic Disease, Justus-Liebig-University Giessen, Benekestr. 2-8, 61231 Bad Nauheim, Germany.
Cells. 2023 May 20;12(10):1432. doi: 10.3390/cells12101432.
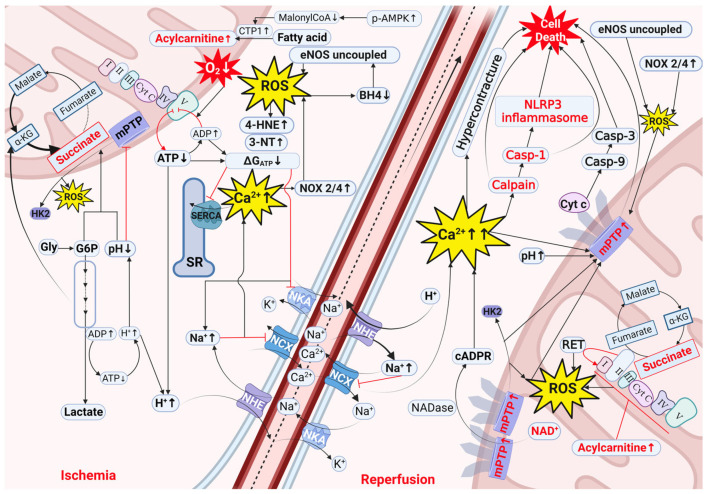
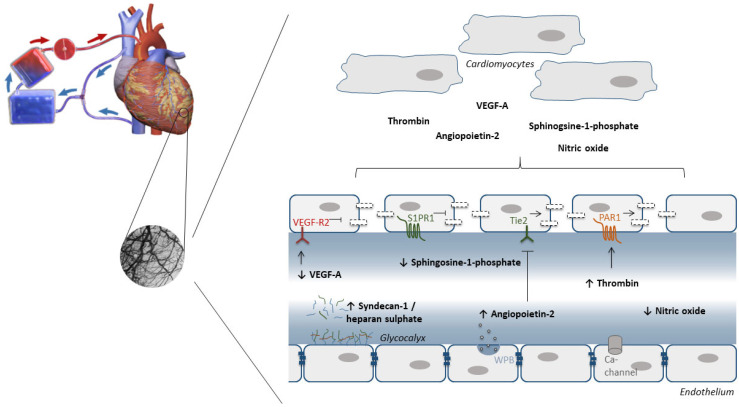
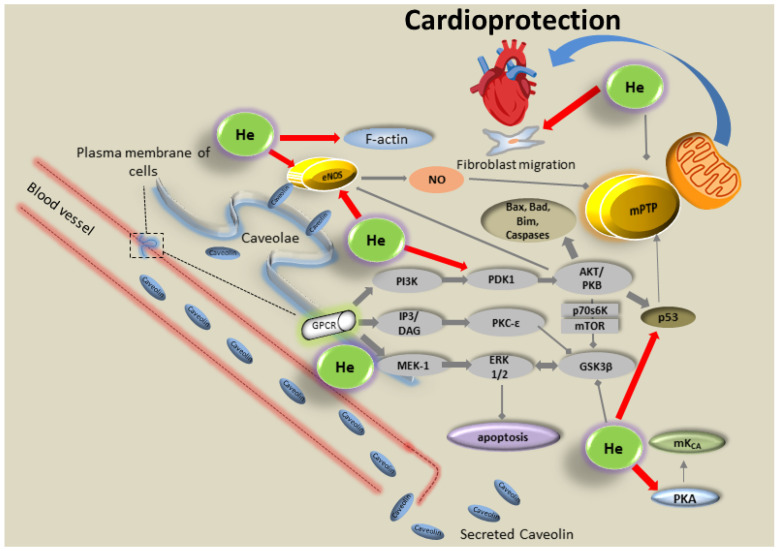
Pharmacological conditioning aims to protect the heart from myocardial ischemia-reperfusion injury (IRI). Despite extensive research in this area, today, a significant gap remains between experimental findings and clinical practice. This review provides an update on recent developments in pharmacological conditioning in the experimental setting and summarizes the clinical evidence of these cardioprotective strategies in the perioperative setting. We start describing the crucial cellular processes during ischemia and reperfusion that drive acute IRI through changes in critical compounds (∆G, Na, Ca, pH, glycogen, succinate, glucose-6-phosphate, mitoHKII, acylcarnitines, BH, and NAD). These compounds all precipitate common end-effector mechanisms of IRI, such as reactive oxygen species (ROS) generation, Ca overload, and mitochondrial permeability transition pore opening (mPTP). We further discuss novel promising interventions targeting these processes, with emphasis on cardiomyocytes and the endothelium. The limited translatability from basic research to clinical practice is likely due to the lack of comorbidities, comedications, and peri-operative treatments in preclinical animal models, employing only monotherapy/monointervention, and the use of no-flow (always in preclinical models) versus low-flow ischemia (often in humans). Future research should focus on improved matching between preclinical models and clinical reality, and on aligning multitarget therapy with optimized dosing and timing towards the human condition.
药理学预处理旨在保护心脏免受心肌缺血再灌注损伤(IRI)。尽管在该领域进行了广泛的研究,但目前,实验发现与临床实践之间仍存在显著差距。本综述提供了在实验环境中关于药理学预处理的最新进展,并总结了这些心脏保护策略在围手术期的临床证据。我们首先描述了在缺血和再灌注过程中驱动急性 IRI 的关键细胞过程,这些过程通过改变关键化合物(∆G、Na、Ca、pH、糖原、琥珀酸、葡萄糖-6-磷酸、线粒体 HKII、酰基辅酶 A、BH 和 NAD)来实现。这些化合物都引发了 IRI 的常见最终效应机制,如活性氧(ROS)生成、Ca 超载和线粒体通透性转换孔(mPTP)开放。我们进一步讨论了针对这些过程的新型有前途的干预措施,重点是心肌细胞和内皮细胞。从基础研究到临床实践的转化有限,可能是由于临床前动物模型中缺乏合并症、合并用药和围手术期治疗,仅采用单一疗法/单一干预,以及使用无血流(始终在临床前模型中)与低血流缺血(经常在人类中)。未来的研究应侧重于改善临床前模型与临床实际情况之间的匹配,并将多靶点治疗与优化剂量和时间与人类状况相协调。