Piening Alexander, Al-Hammadi Noor, Dombrowski John, Hamilton Zachary, Teague Ryan M, Swaminath Anand, Shahi Jeevin
Department of Molecular Microbiology and Immunology, Saint Louis University School of Medicine, St. Louis, Missouri.
Department of Health and Clinical Outcomes Research, AHEAD Institute, Saint Louis University School of Medicine, St. Louis, Missouri.
Adv Radiat Oncol. 2023 Apr 10;8(5):101238. doi: 10.1016/j.adro.2023.101238. eCollection 2023 Sep-Oct.
Immunotherapy (IO) has significantly improved outcomes in metastatic renal cell carcinoma (mRCC). Preclinical evidence suggests that responses to IO may be potentiated via immunomodulatory effects of stereotactic radiation therapy (SRT). We hypothesized that clinical outcomes from the National Cancer Database (NCDB) would demonstrate improved overall survival (OS) in patients with mRCC receiving IO + SRT versus IO alone.
Patients with mRCC receiving first-line IO ± SRT were identified from the NCDB. Conventional radiation therapy was allowed in the IO alone cohort. The primary endpoint was OS stratified by the receipt of SRT (IO + SRT vs IO alone). Secondary endpoints included OS stratified by the presence of brain metastases (BM) and timing of SRT (before or after IO). Survival was estimated using Kaplan-Meier methodology and compared via the log-rank test.
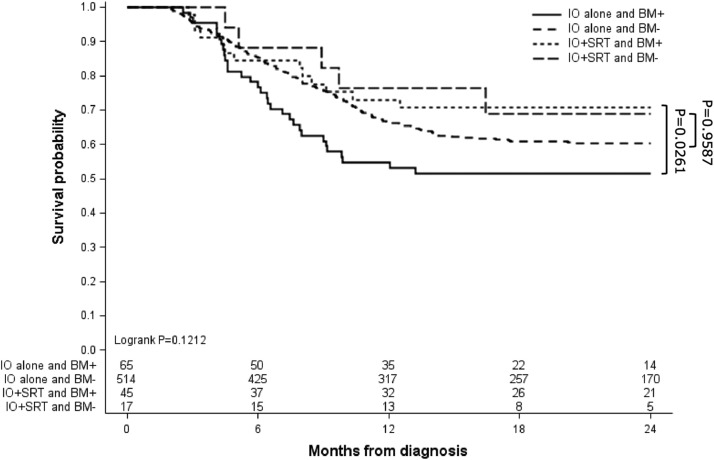
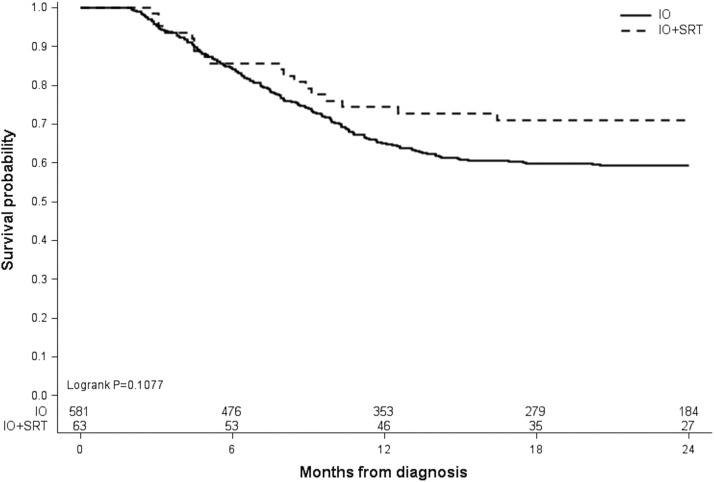
Of 644 eligible patients, 63 (9.8%) received IO + SRT, and 581 (90.2%) received IO alone. Median follow-up time was 17.7 months (range, 2-24 months). Sites treated with SRT included the brain (71.4%), lung/chest (7.9%), bones (7.9%), spine (6.3%), and other (6.3%). OS was 74.4% versus 65.0% at 1 year and 71.0% versus 59.4% at 2 years for the IO + SRT and IO alone groups, respectively, although this difference did not reach statistical significance (log-rank = .1077). In patients with BM, however, 1-year OS (73.0% vs 54.7%) and 2-year OS (70.8% vs 51.4%) was significantly higher in those receiving IO + SRT versus IO alone, respectively (pairwise = .0261). Timing of SRT (before or after IO) did not influence OS (log-rank = .3185).
Patients with BM secondary to mRCC had prolonged OS with the addition of SRT to IO. Factors such as International mRCC Database Consortium risk stratification, oligometastatic tumor burden, SRT dose/fractionation, and utilization of doublet therapy should be considered in future analyses to better identify patients who may benefit from combined IO + SRT. Further prospective studies are warranted.
免疫疗法(IO)显著改善了转移性肾细胞癌(mRCC)的治疗效果。临床前证据表明,立体定向放射治疗(SRT)的免疫调节作用可能增强对IO的反应。我们假设,国家癌症数据库(NCDB)的临床结果将显示,接受IO + SRT的mRCC患者与单纯接受IO的患者相比,总生存期(OS)有所改善。
从NCDB中识别出接受一线IO ± SRT的mRCC患者。单纯IO组允许进行传统放射治疗。主要终点是根据是否接受SRT(IO + SRT与单纯IO)分层的OS。次要终点包括根据脑转移(BM)的存在情况和SRT的时间(IO之前或之后)分层的OS。使用Kaplan-Meier方法估计生存期,并通过对数秩检验进行比较。
在644例符合条件的患者中,63例(9.8%)接受了IO + SRT,581例(90.2%)单纯接受IO。中位随访时间为17.7个月(范围2 - 24个月)。接受SRT治疗的部位包括脑(71.4%)、肺/胸部(7.9%)、骨(7.9%)、脊柱(6.3%)和其他部位(6.3%)。IO + SRT组和单纯IO组的1年OS分别为74.4%和65.0%,2年OS分别为71.0%和59.4%,尽管这种差异未达到统计学意义(对数秩 = 0.1077)。然而,在有BM的患者中,接受IO + SRT的患者1年OS(73.0%对54.7%)和2年OS(70.8%对51.4%)分别显著高于单纯接受IO的患者(配对 = 0.0261)。SRT时间(IO之前或之后)不影响OS(对数秩 = 0.3185)。
继发于mRCC的BM患者在IO基础上加用SRT可延长OS。未来分析中应考虑国际mRCC数据库联盟风险分层、寡转移肿瘤负荷、SRT剂量/分割以及双联疗法的使用等因素,以更好地识别可能从IO + SRT联合治疗中获益的患者。有必要进行进一步的前瞻性研究。