Nguyen Eric K, Lalani Aly Khan A, Ghosh Sunita, Basappa Naveen S, Kapoor Anil, Hansen Aaron R, Kollmannsberger Christian, Heng Daniel, Wood Lori A, Castonguay Vincent, Soulières Denis, Winquist Eric, Canil Christina, Graham Jeffrey, Bjarnason Georg A, Breau Rodney H, Pouliot Frédéric, Swaminath Anand
McMaster University, Hamilton, Ontario, Canada.
Cross Cancer Institute, Edmonton, Alberta, Canada.
Adv Radiat Oncol. 2022 Jan 16;7(4):100899. doi: 10.1016/j.adro.2022.100899. eCollection 2022 Jul-Aug.
With the integration of immunotherapy (IO) agents in the management of metastatic renal cell carcinoma (mRCC), there has been interest in the combined use with radiation therapy (RT). However, real world data are limited. The purpose of this study was to evaluate outcomes in patients with mRCC receiving both RT and IO compared with IO alone.
Data were collected from Canadian Kidney Cancer Information System from January 2011 to September 2019 across 14 academic centers. Patients with mRCC who received IO as first- or second-line therapy were included. RT was categorized as radical dose or palliative dose. Kaplan-Meier estimates were reported for overall survival (OS) and time to treatment failure. Cox proportional hazard models were used adjusted for age and International Metastatic RCC Database Consortium risk categories.
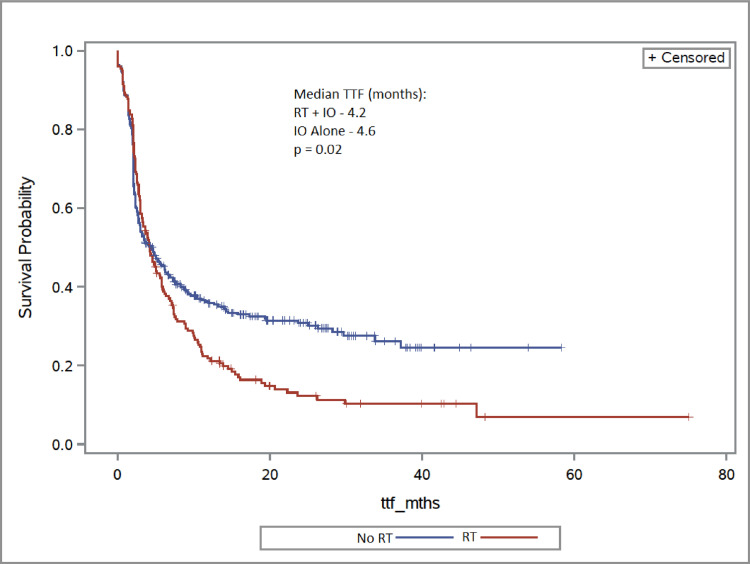
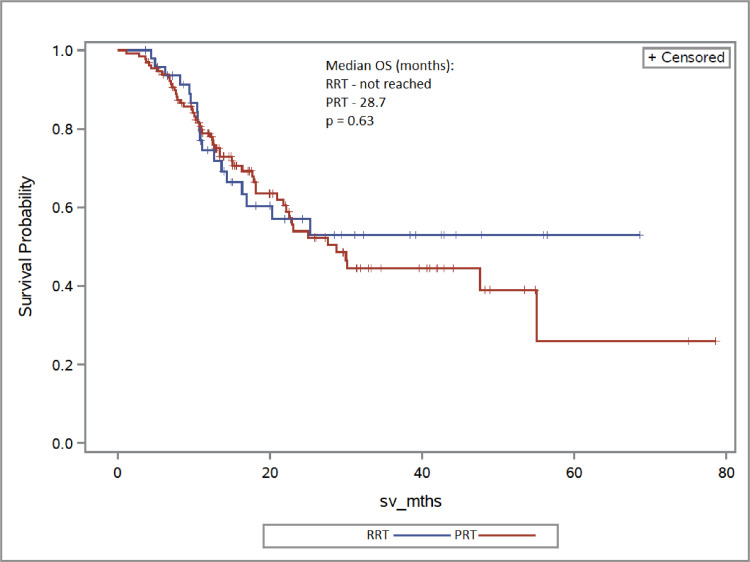
In total, 505 patients were included in the study: 179 received RT + IO and 326 received IO alone. Two-year OS for the RT + IO group was 55.0% compared with 66.4% in the IO alone cohort (adjusted hazard ratio [aHR], 1.38; = .07). At 2 years, 12.2% of the RT + IO patients remained on therapy versus 30.9% in the IO alone group (aHR, 1.30; = .02). For patients receiving first-line therapy, 2-year OS in the RT + IO group was 56.4% versus 78.4% in the IO alone arm, though this difference was not statistically significant (aHR, 1.23; = .56). For patients receiving radical dose and palliative dose, 2-year OS was 57.0% and 53.9%, respectively (aHR, 0.86; = .63).
In this descriptive analysis, more than one-third of patients with mRCC received RT and demonstrated inferior outcomes compared with IO alone. Potential explanations include greater presence of adverse metastatic sites in those receiving RT. Prospective clinical trials evaluating potential benefits of RT in an IO era remain an important need.
随着免疫治疗(IO)药物被纳入转移性肾细胞癌(mRCC)的治疗方案中,人们对其与放射治疗(RT)联合使用产生了兴趣。然而,真实世界的数据有限。本研究的目的是评估接受RT和IO联合治疗的mRCC患者与单纯接受IO治疗的患者的疗效。
收集了2011年1月至2019年9月期间来自加拿大14个学术中心的肾癌信息系统的数据。纳入了接受IO作为一线或二线治疗的mRCC患者。RT分为根治性剂量或姑息性剂量。报告了总生存期(OS)和治疗失败时间的Kaplan-Meier估计值。使用Cox比例风险模型对年龄和国际转移性RCC数据库联盟风险类别进行了调整。
本研究共纳入505例患者:179例接受RT + IO治疗,326例单纯接受IO治疗。RT + IO组的两年OS率为55.0%,而单纯IO组为66.4%(调整后风险比[aHR],1.38;P = 0.07)。两年时,RT + IO组中有12.2%的患者仍在接受治疗,而单纯IO组为30.9%(aHR,1.30;P = 0.02)。对于接受一线治疗的患者,RT + IO组的两年OS率为56.4%,而单纯IO组为78.4%,尽管这种差异无统计学意义(aHR,1.23;P = 0.56)。对于接受根治性剂量和姑息性剂量的患者,两年OS率分别为57.0%和53.9%(aHR,0.86;P = 0.63)。
在这项描述性分析中,超过三分之一的mRCC患者接受了RT治疗,与单纯接受IO治疗相比,疗效较差。可能的解释包括接受RT治疗的患者中不良转移部位更多。在IO时代评估RT潜在益处的前瞻性临床试验仍然非常必要。