Department of Medicine, Section of Cardiology, The University of Chicago Medical Center, Chicago, Illinois.
Department of Medicine, Section of Cardiology, The University of Chicago Medical Center, Chicago, Illinois.
Am J Cardiol. 2023 Sep 1;202:12-16. doi: 10.1016/j.amjcard.2023.06.022. Epub 2023 Jul 4.
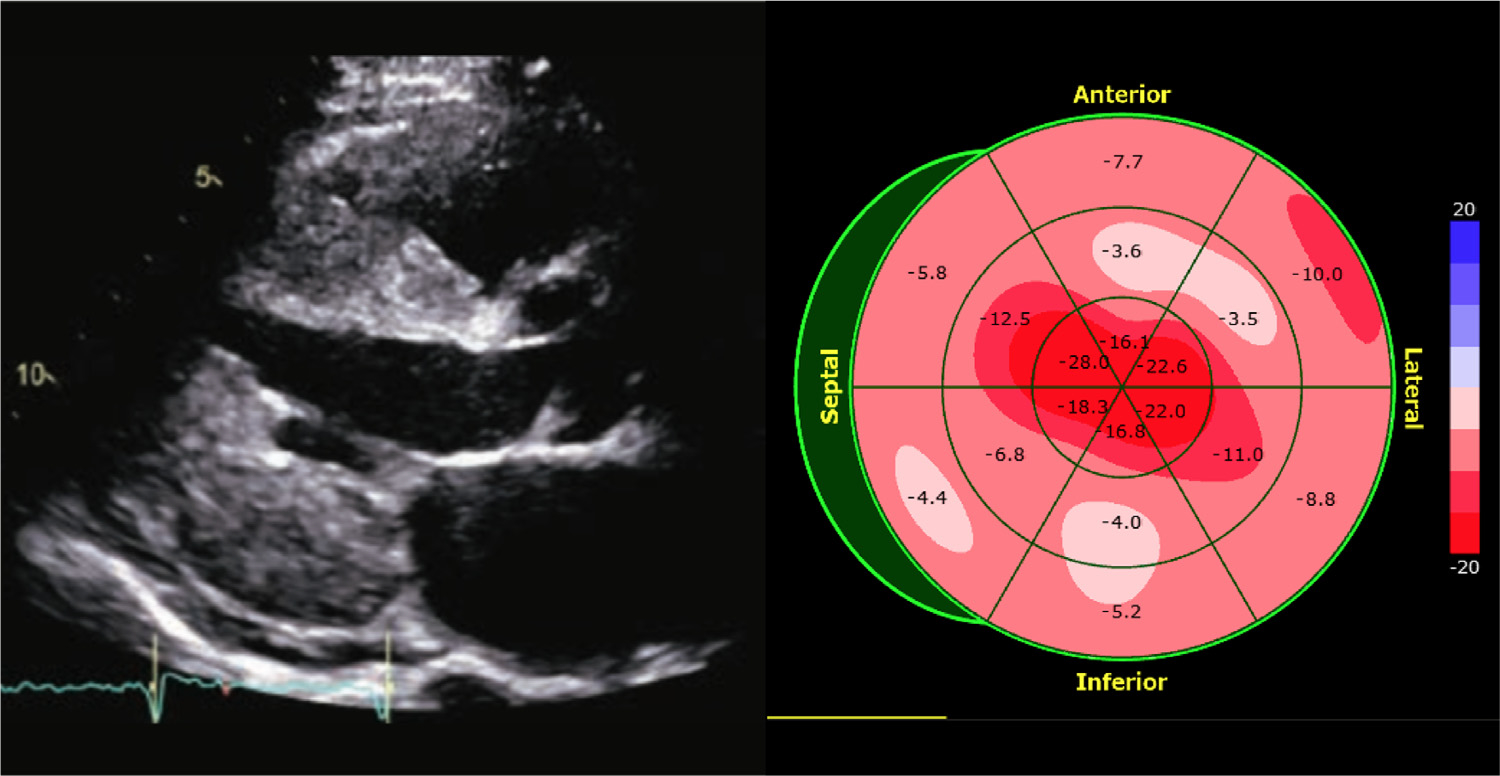
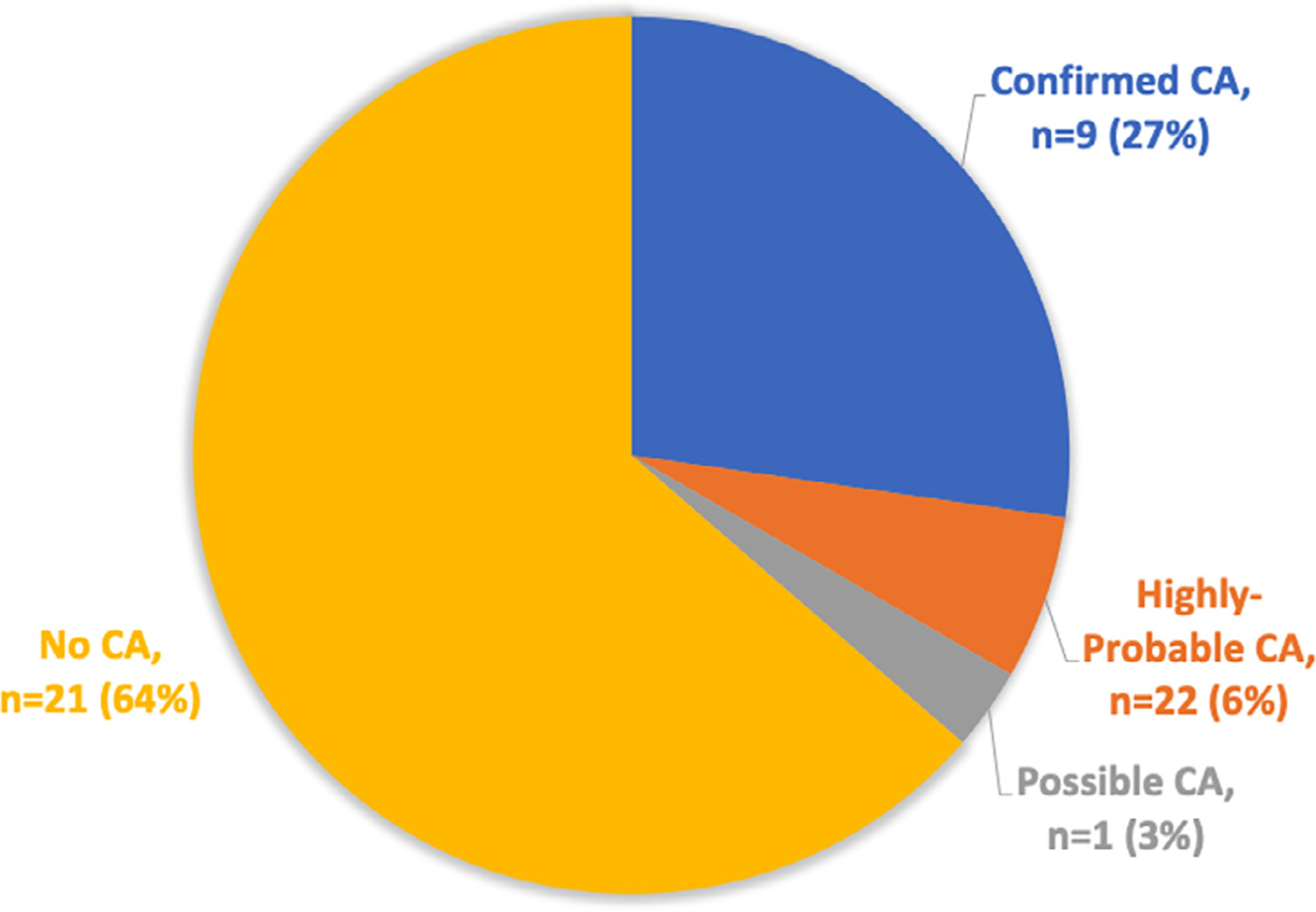
Echocardiographic diagnosis of cardiac amyloidosis (CA) is frequently suggested by the presence of a left ventricular (LV) apical sparing pattern (ASP) on longitudinal strain (LS) assessment, the so-called "cherry on top" pattern, defined by strain magnitude preserved exclusively at the apex. However, it is unclear how frequently this strain pattern truly represents CA. This study aimed to evaluate the predictive value of ASP in the diagnosis of CA. We retrospectively identified consecutive adult patients who had the following studies performed within an 18-month period: (1) transthoracic echocardiogram and (2) either (a) cardiac magnetic resonance imaging, (b) Technetium-Pyrophosphate (PYP) imaging, or (c) endomyocardial biopsy. LS was retrospectively measured in the apical 4-, 3-, and 2-chamber views in patients who had adequate noncontrast images (n = 466). An apical sparing ratio (ASR) was calculated as (average apical strain)/[(average basal strain) + (average midventricular strain)]. Patients with ASR ≥1 were evaluated for the presence/absence of CA, using established criteria. Basic LV parameters were also measured. A total of 33 patients (7.1%) had ASP. Nine of these patients (27%) had "confirmed" CA, 2 (6.1%) "highly probable" CA, 1 (3.0%) "possible" CA, and 21 (64%) no evidence of CA. When comparing patients with and without confirmed CA, there were no significant differences in ASR, average global LS, ejection fraction, or LV mass. Patients with confirmed CA were older (76 ± 9 vs 59 ± 18 years, p = 0.01) and had thicker posterior wall (15 ± 3 vs 11 ± 3 mm, p = 0.004) with a trend toward thicker septal wall (15 ± 2 vs 12 ± 4 mm, p = 0.05). In conclusion, the presence of ASP on LS represents confirmed or highly probable CA in only 1/3 of patients and is more likely to indicate true CA in older patients with increased LV wall thickness. Although a larger, prospective study is needed to confirm these findings, 1/3 should be considered as a large diagnostic yield that justifies further testing, given the poor outcomes associated with CA diagnosis.
超声心动图诊断心脏淀粉样变性(CA)时,通常根据纵向应变(LS)评估存在左心室(LV)心尖保留模式(ASP),即所谓的“樱桃在顶部”模式,由尖端处仅保留的应变幅度定义。然而,目前尚不清楚这种应变模式实际上有多少真正代表 CA。本研究旨在评估 ASP 在 CA 诊断中的预测价值。我们回顾性地确定了在 18 个月内进行了以下研究的连续成年患者:(1)经胸超声心动图和(2)心脏磁共振成像(a)、(b)焦磷酸盐(PYP)成像或(c)心内膜心肌活检。在有足够非对比图像的患者中(n=466),在心尖 4、3 和 2 腔视图中回顾性测量 LS。计算心尖保留比(ASR)为(平均心尖应变)/[(平均基底应变)+(平均中隔应变)]。对于 ASR≥1 的患者,使用既定标准评估 CA 的存在/不存在。还测量了基本的 LV 参数。共有 33 名患者(7.1%)存在 ASP。这些患者中有 9 名(27%)患有“确诊”CA、2 名(6.1%)患有“高度可能”CA、1 名(3.0%)患有“可能”CA 和 21 名(64%)无 CA 证据。比较有和无确诊 CA 的患者,ASR、平均整体 LS、射血分数或 LV 质量无显著差异。确诊 CA 的患者年龄较大(76±9 岁比 59±18 岁,p=0.01),后壁较厚(15±3 毫米比 11±3 毫米,p=0.004),间隔壁较厚(15±2 毫米比 12±4 毫米,p=0.05)有趋势。总之,LS 上的 ASP 仅代表确诊或高度可能的 CA 在 1/3 的患者中,在 LV 壁增厚的老年患者中更可能表示真正的 CA。尽管需要更大的前瞻性研究来证实这些发现,但鉴于 CA 诊断相关的不良结局,1/3 应被视为较大的诊断收益,需要进一步检测。