Department of Biomedical and Clinical Sciences, Division of Inflammation and Infection/Rheumatology, Linköping University, Linköping, Sweden.
Department of Clinical Sciences Lund, Rheumatology, Lund University, Lund, Sweden.
Rheumatology (Oxford). 2024 Apr 2;63(4):1104-1112. doi: 10.1093/rheumatology/kead348.
Patients with SLE have an increased risk of comorbidities and impaired survival. We aimed to assess whether various thresholds of oral CS (OCS) can predict development of infections, comorbidities, malignancies and survival in SLE using data from national health registries in Sweden.
All incident SLE cases, age >18 years, in Sweden (n = 5309) between 2005 and 2020 and matched population controls (n = 26 545) were included and followed until 2020, a total of 257 942 patient years. Data from national registers were retrieved including information from the National Prescribed Drug Register. Risk factors were analysed using time-dependent Cox regression models.
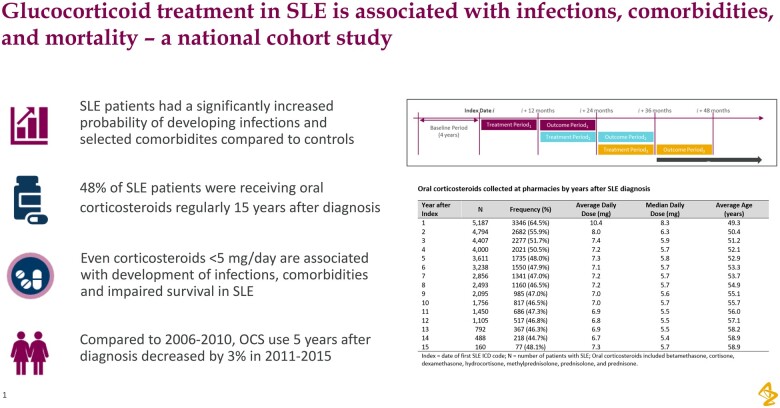
Compared with no OCS, >0 to <5.0 mg/day, 5.0-7.5 mg/day as well as >7.5 mg/day OCS predicted development of infections (pneumonia, influenza, herpes zoster and urinary tract infection), osteoporosis, osteonecrosis, gastroduodenal ulcers, cataracts, hypertension and mortality (all P < 0.05). OCS >0 to <5.0 mg/day was associated with lower hazard ratios for these comorbidities than higher doses of OCS. Fifteen years after diagnosis, 48% of patients were taking OCS at a median dose of 5.7 mg/day. A small reduction of OCS treatment 5 years after diagnosis in patients diagnosed with SLE 2006-10 compared with 2011-15 was observed, 49% vs 46% respectively (P = 0.039).
Results highlight the potential harm associated with even low OCS dose treatment in SLE and the need to judiciously use OCS at the lowest possible dose to maximize efficacy and minimize harm.
患有 SLE 的患者存在合并症风险增加和生存受损的风险。我们旨在使用来自瑞典国家健康登记处的数据评估各种口服皮质类固醇(OCS)阈值是否可以预测 SLE 患者感染、合并症、恶性肿瘤和生存情况。
本研究纳入了 2005 年至 2020 年期间瑞典年龄>18 岁的所有新确诊 SLE 病例(n=5309)和匹配的人群对照(n=26545),并随访至 2020 年,共 257942 人年。从国家登记处检索数据,包括国家处方药物登记处的信息。使用时间依赖性 Cox 回归模型分析危险因素。
与无 OCS 相比,>0 至<5.0mg/天、5.0-7.5mg/天和>7.5mg/天的 OCS 预测了感染(肺炎、流感、带状疱疹和尿路感染)、骨质疏松症、骨坏死、胃十二指肠溃疡、白内障、高血压和死亡率(均 P<0.05)的发生。与较高剂量的 OCS 相比,OCS >0 至<5.0mg/天与这些合并症的较低风险比相关。诊断后 15 年,48%的患者以 5.7mg/天的中位数剂量服用 OCS。与 2011-15 年相比,2006-10 年诊断的 SLE 患者在诊断后 5 年 OCS 治疗量略有减少,分别为 49%和 46%(P=0.039)。
结果突出了即使低剂量 OCS 治疗也与 SLE 相关的潜在危害,需要谨慎使用尽可能低的 OCS 剂量,以最大程度地提高疗效和最小化危害。