Baisden Jamie L, Varghese Vicky, Banerjee Anjishnu, Yoganandan Narayan
Department of Neurosurgery, Medical College of Wisconsin, 8701 Watertown Plank Rd, Milwaukee, WI 53226, United States.
Department of Orthopedics, Skokie Hospital, NorthShore University Health System, 9600 Gross Point Rd, Skokie, IL 60076, United States.
N Am Spine Soc J. 2023 May 11;14:100228. doi: 10.1016/j.xnsj.2023.100228. eCollection 2023 Jun.
Our elderly population is growing and the number of spine fractures in the elderly is also growing. The elderly population in general may be considered as poor surgical candidates experience a high rate of fractures at C1 and C2 compared with the general population. Nonoperative management of upper cervical fractures is not benign as there is a high nonunion rate for both C1 and C2 fractures in the elderly, and orthosis compliance is often suboptimal, or complicated by skin breakdown. The optimal technique for upper cervical stabilization in the elderly may be different than in younger populations as the bone quality is inferior in the elderly. The objective of this basic science study is to determine whether the bone mineral density (BMD) of C1 and C2 vary by region, and if this is a gender difference in this elderly age group.
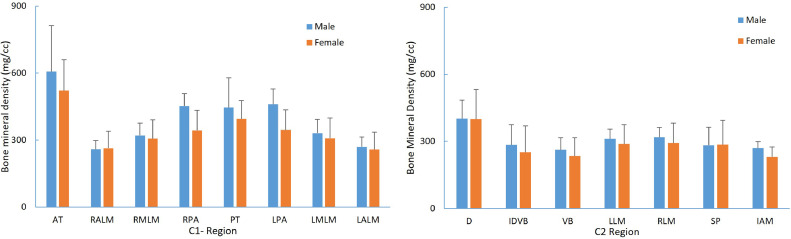
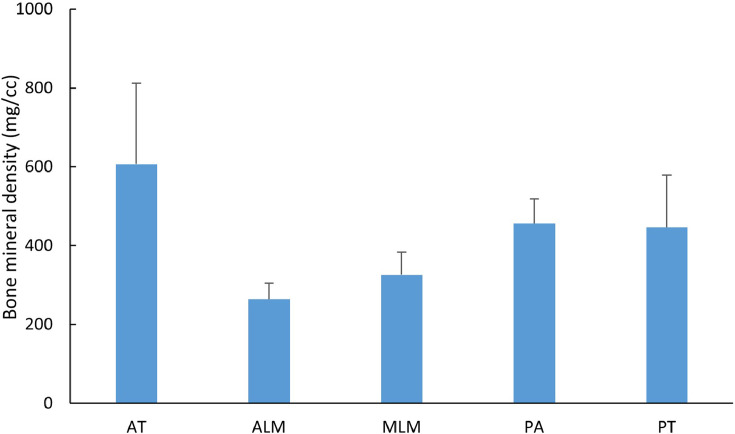
Twenty cadaveric spines from 45 to 83 years of age were used to obtain BMD using quantitated computed tomography (QCT). BMD was measured using a QCT. For C1, 8 regions were determined: anterior tubercle, bilateral anterior and medial lateral masses, bilateral posterior arches, and posterior tubercle. For C2, 7 regional BMDs were determined: top of odontoid, base of odontoid-body interface, mid body, bilateral lateral masses, anterior inferior body near the discs space, and the C2 spinous process.
The BMD was greatest at the C1 anterior tubercle (564.4±175.8 mg/cm) and C1 posterior ring (420.8±110.2 mg/cm), and least at the anterior and medial lateral masses (262.8±59.5 mg/cm, 316.9±72.6 mg/cm). At C2 QCT BMD was greatest at the top of the dens (400.6±107.9 mg/cm) decreasing down through the odontoid-C2 body junction (267.8±103.5 mg/cm) and least in the mid C2 body 249.1±68.8 mg/cm). The posterior arch of C1 and the spinous process of C2 had higher BMD's 420.8±110.2 mg/cm and 284.1±93.0 mg/cm, respectively. A high correlation was observed between the BMD at the interface of the dens-vertebral body with the vertebral body with a Pearson correlation coefficient of 0.86. The BMD of the top of dens was significantly higher (p<.05) than all the regions in C2.
Regional and segmental BMD variations at C1 and C2 have clinical implications for surgical constructs in the elderly population. Given the higher BMDs of the C1 and C2 spinous process and posterior arches, consideration should be given to incorporate these areas using various C1-C2 wiring techniques. In the elderly, lateral masses particularly at C1 with lower BMD may result in potential screw loosening and nonunion in this age group. Old-school wiring techniques have a track record of efficacy and safety with less blood loss, reduced operative time, reduced X-ray exposure, and should be considered in the elderly as a primary stabilization technique or a belt-over suspenders approach based on regional variations in BMD in the elderly.
我们的老年人口正在增长,老年人脊柱骨折的数量也在增加。一般来说,老年人群体可能被视为手术候选不佳者,与普通人群相比,他们在C1和C2处的骨折发生率较高。老年患者上颈椎骨折的非手术治疗并非无害,因为老年患者C1和C2骨折的不愈合率很高,而且矫形器的依从性往往不理想,或者会并发皮肤破损。由于老年人的骨质较差,老年人上颈椎稳定的最佳技术可能与年轻人群体不同。这项基础科学研究的目的是确定C1和C2的骨密度(BMD)是否因区域而异,以及在这个老年年龄组中是否存在性别差异。
使用20具年龄在45至83岁之间的尸体脊柱,通过定量计算机断层扫描(QCT)获得骨密度。使用QCT测量骨密度。对于C1,确定了8个区域:前结节、双侧前外侧块和后外侧块、双侧后弓以及后结节。对于C2,确定了7个区域的骨密度:齿突顶部、齿突-椎体界面底部、椎体中部、双侧侧块、椎间盘间隙附近的椎体前下部以及C2棘突。
C1前结节(564.4±175.8mg/cm)和C1后环(420.8±110.2mg/cm)的骨密度最高,前外侧块和后外侧块(262.8±59.5mg/cm,316.9±72.6mg/cm)的骨密度最低。在C2,QCT骨密度在齿突顶部(400.6±107.9mg/cm)最高,向下穿过齿突-C2椎体交界处(267.8±103.5mg/cm)逐渐降低,在C2椎体中部最低(249.1±68.8mg/cm)。C1后弓和C2棘突的骨密度较高,分别为420.8±110.2mg/cm和284.1±93.0mg/cm。在齿突-椎体界面处的骨密度与椎体骨密度之间观察到高度相关性,皮尔逊相关系数为0.86。齿突顶部的骨密度显著高于C2的所有区域(p<0.05)。
C1和C2的区域和节段性骨密度变化对老年人群体的手术构建具有临床意义。鉴于C1和C2棘突及后弓的骨密度较高,应考虑使用各种C1-C2钢丝技术将这些区域纳入。在老年人中,特别是C1处骨密度较低的侧块可能导致该年龄组潜在的螺钉松动和不愈合。传统的钢丝技术有疗效和安全性记录,失血少、手术时间短、X线暴露减少,应将其作为老年患者的主要稳定技术或基于老年人骨密度区域差异的双重保险方法加以考虑。