Lau Brianna, Tominez Paul, Shing Jaimie Z, Vo Jacqueline B, Pollom Erqi, Taparra Kekoa
Department of Radiation Oncology, Stanford Medicine, Palo Alto, CA 94304, USA.
School of Medicine, University of California, San Francisco, CA 94143, USA.
Cancers (Basel). 2023 Jun 26;15(13):3358. doi: 10.3390/cancers15133358.
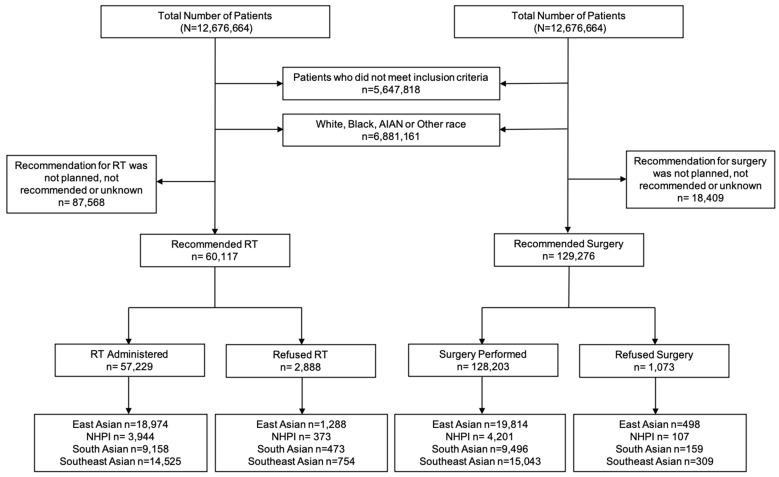
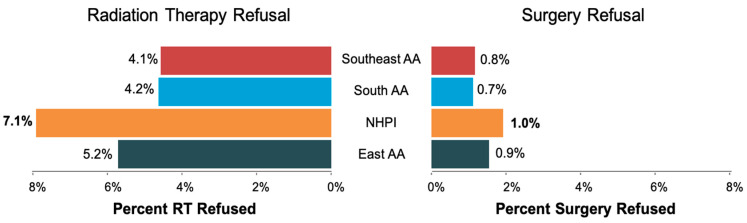
Despite radiation therapy (RT) and surgery being the curative treatments, prior work demonstrated that the aggregated Asian American (AA) and Native Hawaiian and Other Pacific Islanders (NHPI) population refuse RT and surgery at a higher rates than other races. Given that AA and NHPI are distinct groups, data disaggregation is necessary to understand racial and ethnic disparities for treatment refusal. We aimed to (1) compare RT and surgery refusal rates between AA and NHPI populations, (2) assess RT and surgery refusal on overall mortality, and (3) determine predictors of refusing RT and surgery using the United States (U.S.) National Cancer Database. Adjusted odds ratios (aOR) and 95% confidence intervals (95%CI) for treatment refusal were calculated using logistic regression. Adjusted hazard ratios (aHR) were calculated for overall survival using Cox proportional hazard models among propensity score-matched groups. The overall rate of RT refusal was 4.8% and surgery refusal was 0.8%. Compared to East AA patients, NHPI patients had the highest risk of both RT refusal (aOR = 1.38, 95%CI = 1.21-1.61) and surgery refusal (aOR = 1.28, 95%CI = 1.00-1.61). RT refusal significantly predicted higher mortality (aHR = 1.17, 95%CI = 1.08-1.27), whereas surgery refusal did not. Predictors of RT and surgery refusal were older patient age, high comorbidity index, and cancer diagnosis between 2011-2017. The results show heterogenous treatment refusal patterns among AA and NHPI populations, suggesting areas for targeted intervention.
尽管放射治疗(RT)和手术是治愈性治疗方法,但先前的研究表明,亚裔美国人(AA)以及夏威夷原住民和其他太平洋岛民(NHPI)群体拒绝接受RT和手术的比例高于其他种族。鉴于AA和NHPI是不同的群体,有必要进行数据分解以了解拒绝治疗方面的种族和民族差异。我们旨在:(1)比较AA和NHPI群体之间的RT和手术拒绝率;(2)评估RT和手术拒绝对总体死亡率的影响;(3)使用美国国家癌症数据库确定拒绝RT和手术的预测因素。使用逻辑回归计算治疗拒绝的调整优势比(aOR)和95%置信区间(95%CI)。在倾向评分匹配组中,使用Cox比例风险模型计算总体生存率的调整风险比(aHR)。RT拒绝的总体率为4.8%,手术拒绝率为0.8%。与东亚裔AA患者相比,NHPI患者拒绝RT(aOR = 1.38,95%CI = 1.21 - 1.61)和手术(aOR = 1.28,95%CI = 1.00 - 1.61)的风险最高。RT拒绝显著预测更高的死亡率(aHR = 1.17,95%CI = 1.08 - 1.27),而手术拒绝则不然。RT和手术拒绝的预测因素包括患者年龄较大、高合并症指数以及2011 - 2017年期间的癌症诊断。结果显示AA和NHPI群体中存在不同的治疗拒绝模式,提示了有针对性干预的领域。