Kokoreva K D, Chugunov I S, Vladimirova V P, Ivannikova T E, Bogdanov V P, Bezlepkina O B
Endocrinology Research Centre.
Probl Endokrinol (Mosk). 2023 May 11;69(2):67-74. doi: 10.14341/probl13216.
The majority of Kallmann patients have anosmia or hyposmia. This is how the disease is diagnosed. Some of them don't have such complaints but olfactory dysfunction is diagnosed via olfactometry. Nowadays there is the lack of information about correlation between olfactometry results and subjective complaints. Correlation between olfactory bulbs size and olfactory dysfunction has been little studied.
To explore olfactory bulb size and olfactory function in patients with congenital isolated hypogonadotropic hypogonadism. To correlate olfactory bulb sizes and smell test scores.
Single-centre comparative study. 34 patients were included. The main group consisted of 19 patients with hypogonadotropic (15 -with Kallmann syndrome, 4 - with normosmic hypogonadism). Olfactory bulbs MRI were provided to all the patients, olfactory test (Sniffin' Sticks Test) and molecular-genetic studies were provided in all patients with hypogonadism. Control group consisted of 15 patients who were provided with orbits MRI. Olfactory bulbs were evaluated additionally in them.
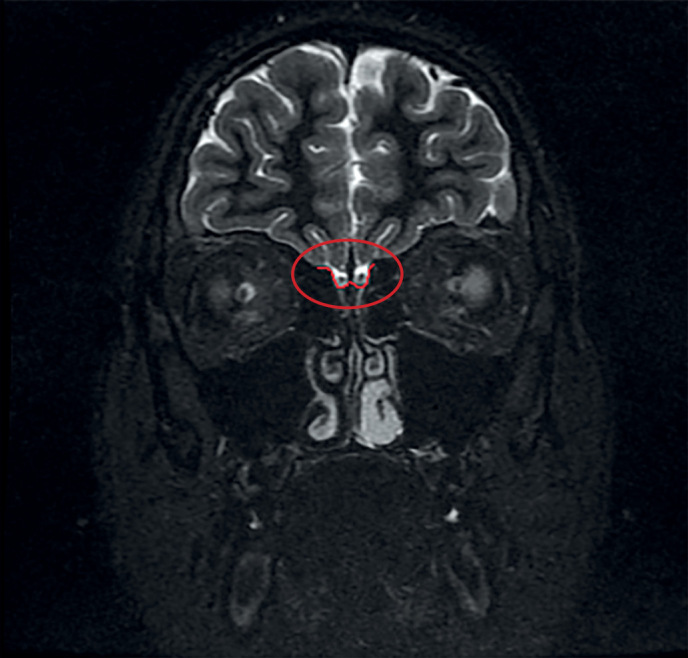
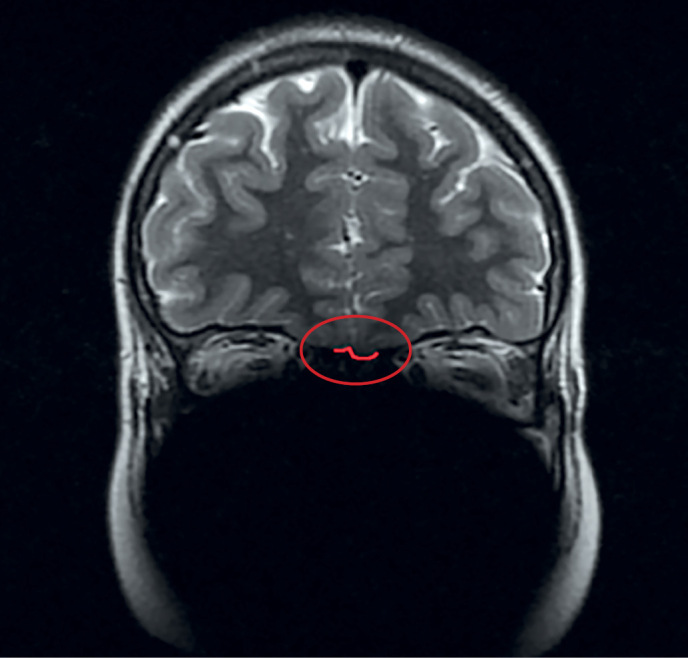
Normal size of olfactory bulbs were only in 1 patient with hypogonadism. Olfactory bulbs height and width were significantly smaller in patients with hypogonadism in comparison with control group (p<0.01). Height median of right bulb was 1.0 mm [0.2; 1.8] in patients from the main group vs. 3.0 [2.5; 3.2] in controls, width median of right bulb was 1.0 mm [0.2; 1.9] in patients from the main group vs. 2.5 [2.0; 3.0] in controls. Height median of left bulb was 0.8 mm [0.0; 1.2] in patients from the main group vs. 3.0 [2.7; 3.2] in controls, width median of left bulb was 0.8 mm [0.0; 1.2] in patients from the main group vs. 2.5 [2.0; 3.0] in controls. Correlation has been established between left bulb height (r=0.59) and width (r=0.67) and olfactometry results (p<0.05). 4 patients had no anosmia complaints but had olfactory dysfunction according to Sniffin' Sticks Tests.
Olfactometry was able to diagnose olfactory dysfunction in 78.5% (i.e. in 15 out of 19 patients with congenital isolated hypogonadotropic hypogonadism. However, anosmia complaints had only 11 out of 19 patients. It is the first results of olfactory bulb sizes in patients with hypogonadotropic hypogonadism in Russia. Uni - or bilateral hypoor aplasia were diagnosed in 94.7% patients with hypogonadism regardless of olfactory dysfunction. Bilateral olfactory bulbs hypoplasia were the most common MRI-finding (36.8%). Unilateral hypoor aplasia was diagnosed in 31.6% patients.
大多数卡尔曼综合征患者存在嗅觉缺失或嗅觉减退,疾病正是据此得以诊断。部分患者并无此类主诉,但通过嗅觉测量法诊断出存在嗅觉功能障碍。目前,关于嗅觉测量结果与主观主诉之间的相关性缺乏相关信息。嗅球大小与嗅觉功能障碍之间的相关性研究较少。
探究先天性孤立性低促性腺激素性性腺功能减退患者的嗅球大小及嗅觉功能,将嗅球大小与嗅觉测试分数进行关联分析。
单中心对照研究。纳入34例患者。主要组由19例低促性腺激素患者组成(15例患有卡尔曼综合征,4例患有嗅觉正常的性腺功能减退症)。对所有患者均进行了嗅球磁共振成像检查,对所有性腺功能减退患者均进行了嗅觉测试(嗅棒测试)及分子遗传学研究。对照组由15例接受眼眶磁共振成像检查的患者组成,并对其嗅球进行了额外评估。
仅1例性腺功能减退患者的嗅球大小正常。与对照组相比,性腺功能减退患者的嗅球高度和宽度明显更小(p<0.01)。主要组患者右侧嗅球高度中位数为1.0毫米[0.2;1.8],而对照组为3.0[2.5;3.2];主要组患者右侧嗅球宽度中位数为1.0毫米[0.2;1.9],而对照组为2.5[2.0;3.0]。主要组患者左侧嗅球高度中位数为0.8毫米[0.0;1.2],而对照组为3.0[2.7;3.2];主要组患者左侧嗅球宽度中位数为0.8毫米[0.0;1.2],而对照组为2.5[2.0;3.0]。已确定左侧嗅球高度(r = 0.59)和宽度(r = 0.67)与嗅觉测量结果之间存在相关性(p<0.05)。4例患者无嗅觉缺失主诉,但根据嗅棒测试存在嗅觉功能障碍。
嗅觉测量法能够诊断出78.5%的嗅觉功能障碍(即19例先天性孤立性低促性腺激素性性腺功能减退患者中的15例)。然而,19例患者中仅有11例有嗅觉缺失主诉。这是俄罗斯关于低促性腺激素性性腺功能减退患者嗅球大小的首批研究结果。94.7%的性腺功能减退患者被诊断为单侧或双侧发育不全或发育不良,无论其是否存在嗅觉功能障碍。双侧嗅球发育不全是最常见的磁共振成像表现(36.8%)。31.6%的患者被诊断为单侧发育不全或发育不良。