Department of Surgical, Oncological and Oral Sciences, Section of Medical Oncology, University of Palermo, Palermo, Italy.
Department of Pharmacy and Biotechnology, University of Bologna, Bologna, Italy.
Oncologist. 2024 Jan 5;29(1):e141-e151. doi: 10.1093/oncolo/oyad206.
The patient selection for optimal adjuvant therapy in gastrointestinal stromal tumors (GISTs) is provided by nomogram based on tumor size, mitotic index, tumor location, and tumor rupture. Although mutational status is not currently used to risk assessment, tumor genotype showed a prognostic influence on natural history and tumor relapse. Innovative measures, such as KIT/PDGFRA-mutant-specific variant allele frequency (VAF) levels detection from next-generation sequencing (NGS), may act as a surrogate of tumor burden and correlate with prognosis and overall survival of patients with GIST, helping the choice for adjuvant treatment.
This was a multicenter, hospital-based, retrospective/prospective cohort study to investigate the prognostic role of KIT or PDGFRA-VAF of GIST in patients with radically resected localized disease. In the current manuscript, we present the results from the retrospective phase of the study.
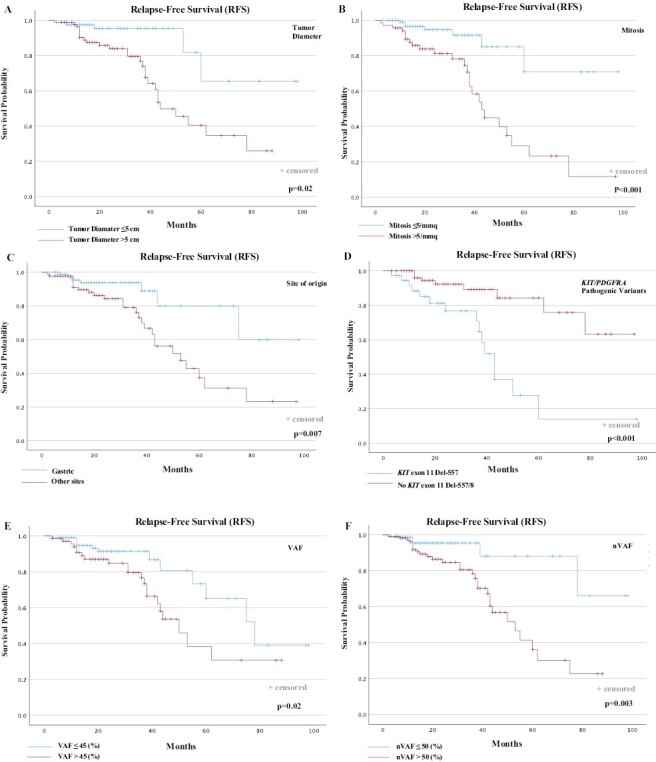
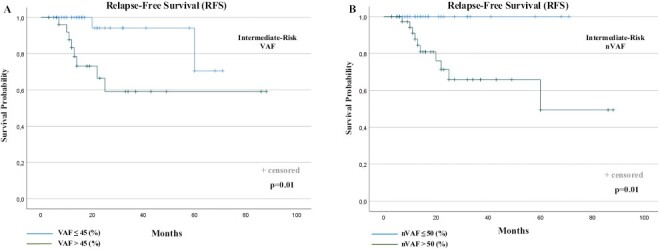
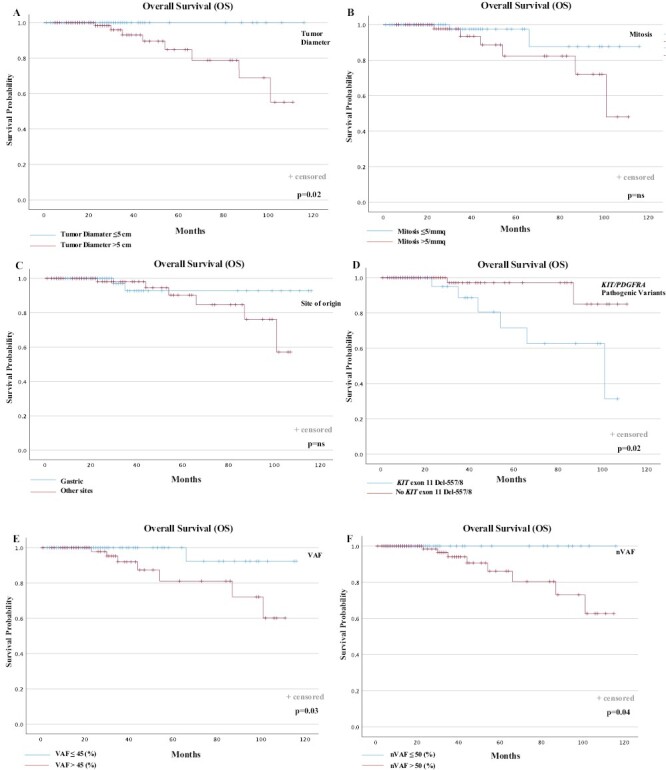
Two-hundred (200) patients with GIST between 2015 and 2022 afferent to 6 Italian Oncologic Centers in the EURACAN Network were included in the study. The receiver operating characteristic (ROC) curves analysis was used to classify "low" vs. "high" VAF values, further normalized on neoplastic cellularity (nVAF). When RFS between the low and high nVAF groups were compared, patients with GIST with KIT/PDGFRA nVAF > 50% showed less favorable RFS than patients in the group of nVAF ≤ 50% (2-year RFS, 72.6% vs. 93%, respectively; P = .003). The multivariable Cox regression model confirmed these results. In the homogeneous sub-population of intermediate-risk, patients with KIT-mutated GIST, the presence of nVAF >50% was statistically associated with higher disease recurrence.
In our study, we demonstrated that higher nVAF levels were independent predictors of GIST prognosis and survival in localized GIST patients with tumors harboring KIT or PDGFRA mutations. In the cohort of intermediate-risk patients, nVAF could be helpful to improve prognostication and the use of adjuvant imatinib.
胃肠道间质瘤(GIST)的最佳辅助治疗患者选择是基于肿瘤大小、有丝分裂指数、肿瘤位置和肿瘤破裂的列线图提供的。尽管突变状态目前不用于风险评估,但肿瘤基因型对自然病史和肿瘤复发有预后影响。创新措施,如从下一代测序(NGS)检测 KIT/PDGFRA 突变特异性变异等位基因频率(VAF)水平,可作为肿瘤负担的替代指标,与 GIST 患者的预后和总生存相关,有助于辅助治疗的选择。
这是一项多中心、基于医院的回顾性/前瞻性队列研究,旨在研究 GIST 中 KIT 或 PDGFRA-VAF 的肿瘤负担与接受根治性局部切除的局限性疾病患者的预后的关系。在本手稿中,我们介绍了该研究回顾性阶段的结果。
2015 年至 2022 年期间,EURACAN 网络的 6 个意大利肿瘤中心共纳入 200 例 GIST 患者。使用受试者工作特征(ROC)曲线分析对“低”与“高”VAF 值进行分类,并进一步对肿瘤细胞密度(nVAF)进行归一化。当比较低和高 nVAF 组之间的 RFS 时,与 nVAF≤50%的组相比,KIT/PDGFRA nVAF>50%的 GIST 患者的 RFS 较差(2 年 RFS,分别为 72.6%和 93%;P=0.003)。多变量 Cox 回归模型证实了这些结果。在 KIT 突变的中间风险亚组患者中,nVAF>50%与更高的疾病复发率有统计学关联。
在我们的研究中,我们证明了在携带 KIT 或 PDGFRA 突变的局限性 GIST 患者中,更高的 nVAF 水平是独立的 GIST 预后和生存的预测因子。在中间风险患者队列中,nVAF 可能有助于改善预后和辅助伊马替尼的使用。