Department of Infectious Diseases, Aarhus University Hospital, Aarhus N, Denmark.
Interdiciplinary Nanoscience Center (iNANO), Aarhus University, Aarhus C, Denmark.
PLoS One. 2023 Jul 18;18(7):e0287671. doi: 10.1371/journal.pone.0287671. eCollection 2023.
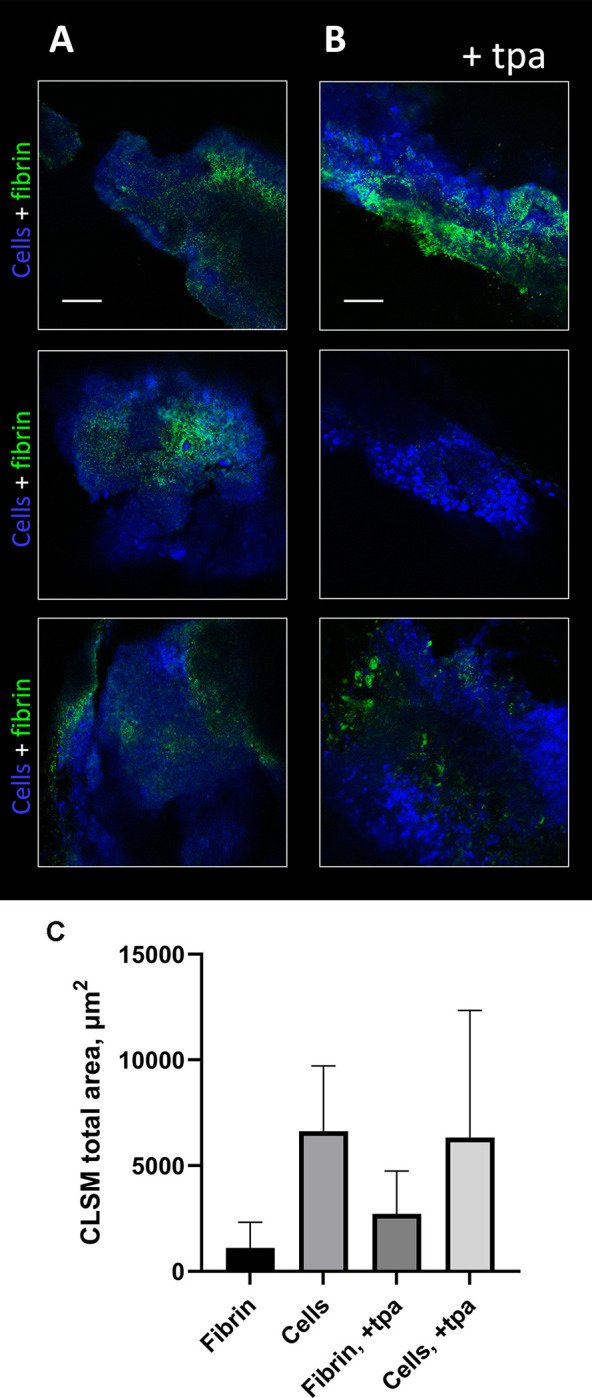
We developed a rat model of prosthetic vascular graft infection to assess, whether the fibrinolytic tissue plasminogen activator (tPA) could increase the efficacy of antibiotic therapy.
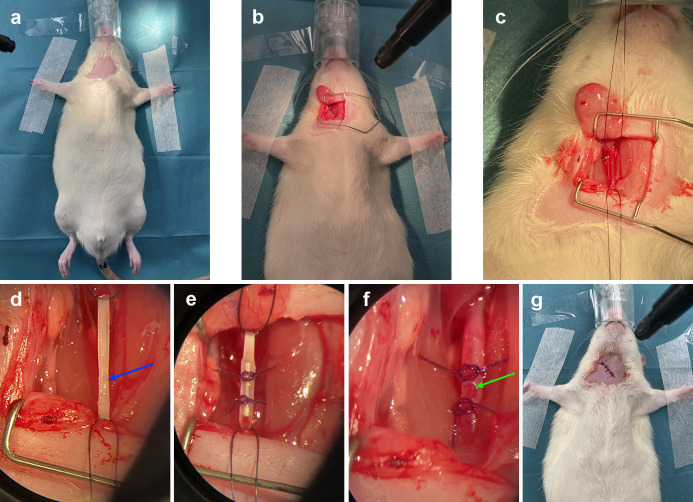
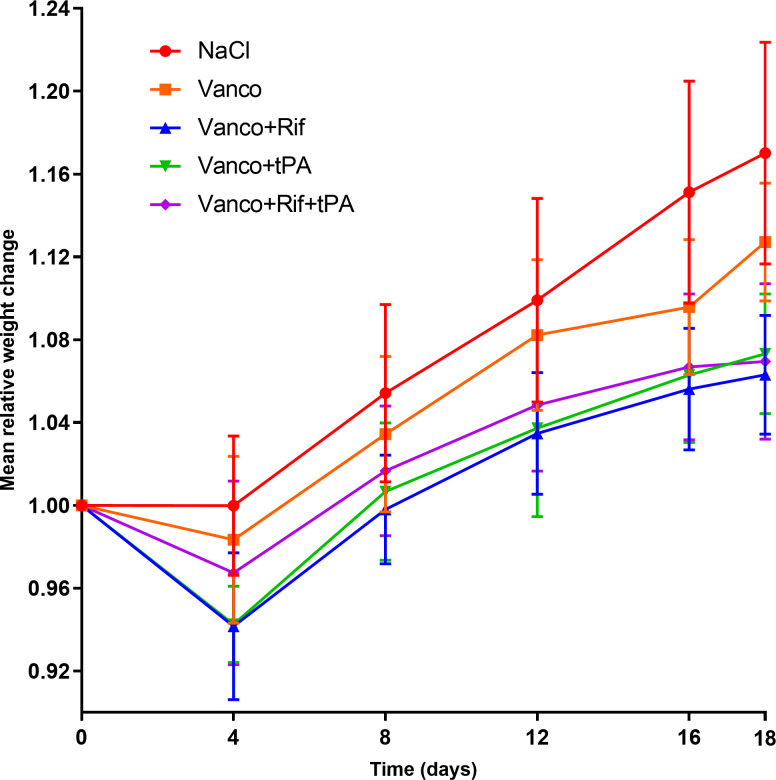
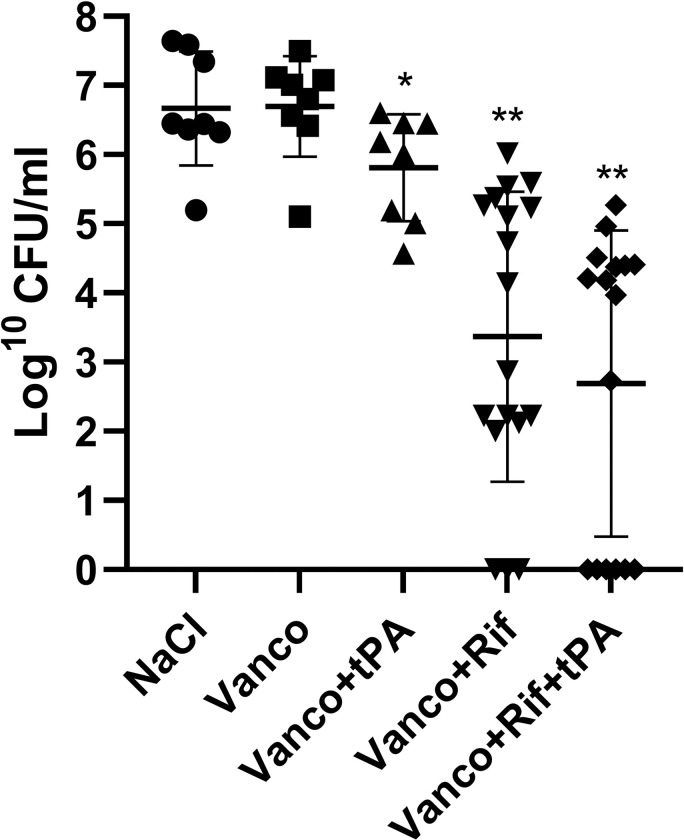
Rats were implanted a polyethylene graft in the common carotid artery, pre-inoculated with approx. 6 log10 colony forming units (CFU) of methicillin resistant Staphylococcus aureus. Ten days after surgery, rats were randomized to either: 0.9% NaCl (n = 8), vancomycin (n = 8), vancomycin + tPA (n = 8), vancomycin + rifampicin (n = 18) or vancomycin + rifampicin + tPA (n = 18). Treatment duration was seven days. Approximately 36 hours after the end of treatment, the rats were euthanized, and grafts and organs were harvested for CFU enumeration.
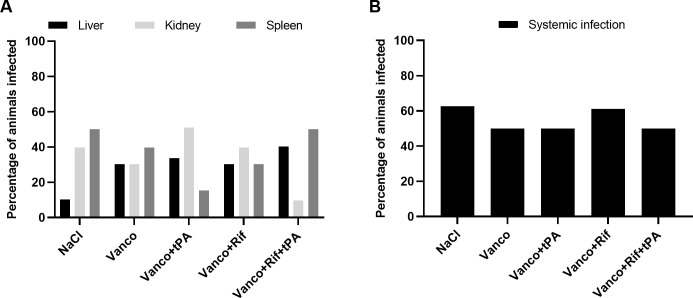
All animals in the control group had significantly higher CFU at the time of euthanization compared to bacterial load found on the grafts prior to inoculation (6.45 vs. 4.36 mean log10 CFU/mL, p = 0.0011), and both the procedure and infection were well tolerated. Vancomycin and rifampicin treatment were superior to monotherapy with vancomycin, as it lead to a marked decrease in median bacterial load on the grafts (3.50 vs. 6.56 log10 CFU/mL, p = 0.0016). The addition of tPA to vancomycin and rifampicin combination treatment did not show a further decrease in bacterial load (4.078 vs. 3.50 log10 CFU/mL, p = 0.26). The cure rate was 16% in the vancomycin + rifampicin group vs. 37.5% cure rate in the vancomycin + rifampicin + tPA group. Whilst interesting, this trend was not significant at our sample size (p = 0.24).
We developed the first functional model of an arterial prosthetic vascular graft infection in rats. Antibiotic combination therapy with vancomycin and rifampicin was superior to vancomycin monotherapy, and the addition of tPA did not significantly reduce bacterial load, nor significantly increase cure rate.
我们建立了一种大鼠人工血管移植物感染模型,以评估纤维蛋白溶解组织型纤溶酶原激活物(tPA)是否能提高抗生素治疗的效果。
大鼠在颈总动脉内置入聚乙烯移植物,预先接种约 6 对数 10 个(CFU)耐甲氧西林金黄色葡萄球菌。手术后 10 天,大鼠随机分为以下几组:0.9%生理盐水(n = 8)、万古霉素(n = 8)、万古霉素+tPA(n = 8)、万古霉素+利福平(n = 18)或万古霉素+利福平+tPA(n = 18)。治疗持续 7 天。治疗结束后约 36 小时,处死大鼠,采集移植物和器官进行 CFU 计数。
与接种前移植物上的细菌负荷(6.45 与 4.36 平均对数 10 CFU/mL,p = 0.0011)相比,对照组所有动物在处死时的 CFU 明显更高,并且手术和感染均得到良好耐受。万古霉素和利福平治疗优于万古霉素单药治疗,因为它显著降低了移植物上的中位细菌负荷(3.50 与 6.56 对数 10 CFU/mL,p = 0.0016)。tPA 联合万古霉素和利福平治疗并未进一步降低细菌负荷(4.078 与 3.50 对数 10 CFU/mL,p = 0.26)。万古霉素+利福平组的治愈率为 16%,而万古霉素+利福平+tPA 组的治愈率为 37.5%。虽然这一趋势很有趣,但在我们的样本量下,这并没有达到统计学意义(p = 0.24)。
我们在大鼠中建立了第一个功能性人工血管移植物感染模型。万古霉素和利福平联合抗生素治疗优于万古霉素单药治疗,而添加 tPA 并未显著降低细菌负荷,也未显著提高治愈率。