Fondazione Policlinico Universitario A. Gemelli IRCCS, Rome, Italy.
Università Cattolica del Sacro Cuore, Largo Agostino Gemelli 8, 00168, Rome, Italy.
Eur Heart J Cardiovasc Imaging. 2023 Dec 21;25(1):48-57. doi: 10.1093/ehjci/jead172.
Despite growing evidence supporting the clinical utility of optical coherence tomography (OCT) guidance during percutaneous coronary interventions (PCIs), there is no common agreement as to the optimal stent implantation parameters that enhance clinical outcome.
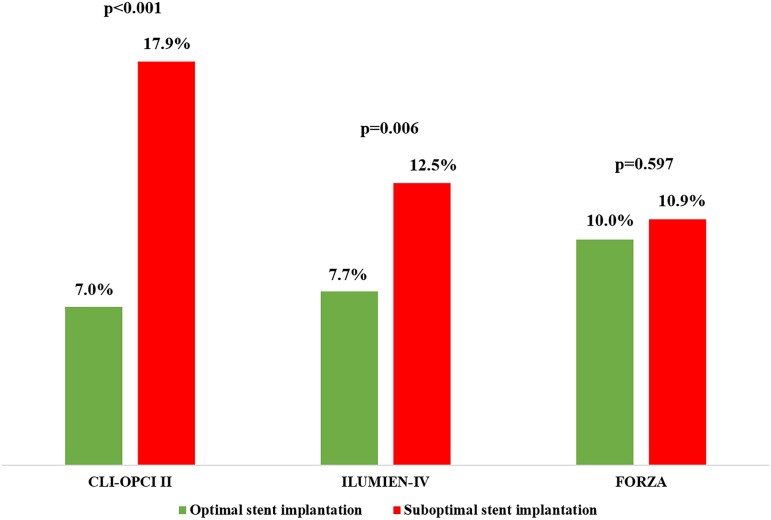
We retrospectively examined the predictive accuracy of suboptimal stent implantation definitions proposed from the CLI-OPCI II, ILUMIEN-IV OPTIMAL PCI, and FORZA studies for the long-term risk of device-oriented cardiovascular events (DoCE) in the population of large all-comers CLI-OPCI project. A total of 1020 patients undergoing OCT-guided drug-eluting stent implantation in the CLI-OPCI registry with a median follow-up of 809 (quartiles 414-1376) days constituted the study population. According to CLI-OPCI II, ILUMIEN-IV OPTIMAL PCI, and FORZA criteria, the incidence of suboptimal stent implantation was 31.8%, 58.1%, and 57.8%, respectively. By multivariable Cox analysis, suboptimal stent implantation criteria from the CLI-OPCI II [hazard ratio 2.75 (95% confidence interval 1.88-4.02), P < 0.001] and ILUMIEN-IV OPTIMAL PCI [1.79 (1.18-2.71), P = 0.006] studies, but not FORZA trial [1.11 (0.75-1.63), P = 0.597], were predictive of DoCE. At long-term follow-up, stent edge disease with minimum lumen area <4.5 mm2 [8.17 (5.32-12.53), P < 0.001], stent edge dissection [2.38 (1.33-4.27), P = 0.004], and minimum stent area <4.5 mm2 [1.68 (1.13-2.51), P = 0.011] were the main OCT predictors of DoCE.
The clinical utility of OCT-guided PCI might depend on the metrics adopted to define suboptimal stent implantation. Uncovered disease at the stent border, stent edge dissection, and minimum stent area <4.5 mm2 were the strongest OCT associates of stent failure.
尽管越来越多的证据支持在经皮冠状动脉介入治疗(PCI)期间使用光学相干断层扫描(OCT)指导,但对于增强临床结果的最佳支架植入参数尚无共识。
我们回顾性地检查了 CLI-OPCI II、ILUMIEN-IV OPTIMAL PCI 和 FORZA 研究中提出的亚最佳支架植入定义在 CLI-OPCI 项目的大所有患者人群中对器械定向心血管事件(DoCE)长期风险的预测准确性。共有 1020 名接受 CLI-OPCI 登记处的 OCT 指导的药物洗脱支架植入的患者,中位随访时间为 809(四分位间距 414-1376)天,构成了研究人群。根据 CLI-OPCI II、ILUMIEN-IV OPTIMAL PCI 和 FORZA 标准,亚最佳支架植入的发生率分别为 31.8%、58.1%和 57.8%。通过多变量 Cox 分析,CLI-OPCI II 中的亚最佳支架植入标准[危险比 2.75(95%置信区间 1.88-4.02),P<0.001]和 ILUMIEN-IV OPTIMAL PCI [1.79(1.18-2.71),P=0.006],但不是 FORZA 试验[1.11(0.75-1.63),P=0.597],可预测 DoCE。在长期随访中,最小管腔面积<4.5mm2 的支架边缘疾病[8.17(5.32-12.53),P<0.001]、支架边缘夹层[2.38(1.33-4.27),P=0.004]和最小支架面积<4.5mm2 [1.68(1.13-2.51),P=0.011]是 DoCE 的主要 OCT 预测指标。
OCT 指导的 PCI 的临床实用性可能取决于用于定义亚最佳支架植入的指标。支架边缘未覆盖病变、支架边缘夹层和最小支架面积<4.5mm2 是支架失败的最强 OCT 关联物。