Hampton Zachary, Davis Alex, Kalnow Andrew
OhioHealth Doctors Hospital, Department of Emergency Medicine, Columbus, OH.
J Educ Teach Emerg Med. 2020 Apr 15;5(2):I1-I8. doi: 10.21980/J8R928. eCollection 2020 Apr.
Three dimensional printed cricothyrotomy trainers are designed to be used at all levels of training in emergency medicine, both for skill acquisition and to prevent skill atrophy.
Simulation has long provided a means to train providers on rarely performed procedures.1,2 For example, surgical cricothyrotomy has commonly been practiced in a simulated environment almost exclusively via low-fidelity models.3-6 What seems to be lacking in this training is simulation of needle cricothyrotomy for the pediatric population. Needle cricothyrotomy remains the standard of care for temporary airway management in a "can't intubate, can't oxygenate" scenario for pediatric patients. In order to address this educational deficiency, we designed a 3D printed pediatric needle cricothyrotomy trainer using evidenced-based cadaveric literature demonstrating neonatal cricothyroid membrane dimensions. These trainers will serve as a simulation tool that will help educate emergency medicine residents to perform a rare, high-stakes procedure within a controlled environment.
By the end of this educational session, participants should be able to:Discuss indications and contraindications for needle cricothyrotomy in the pediatric population.Assemble the equipment needed to complete a needle cricothyrotomy.Describe and perform the steps of neonatal and pediatric needle cricothyrotomy.Discuss post-procedure ventilation options.
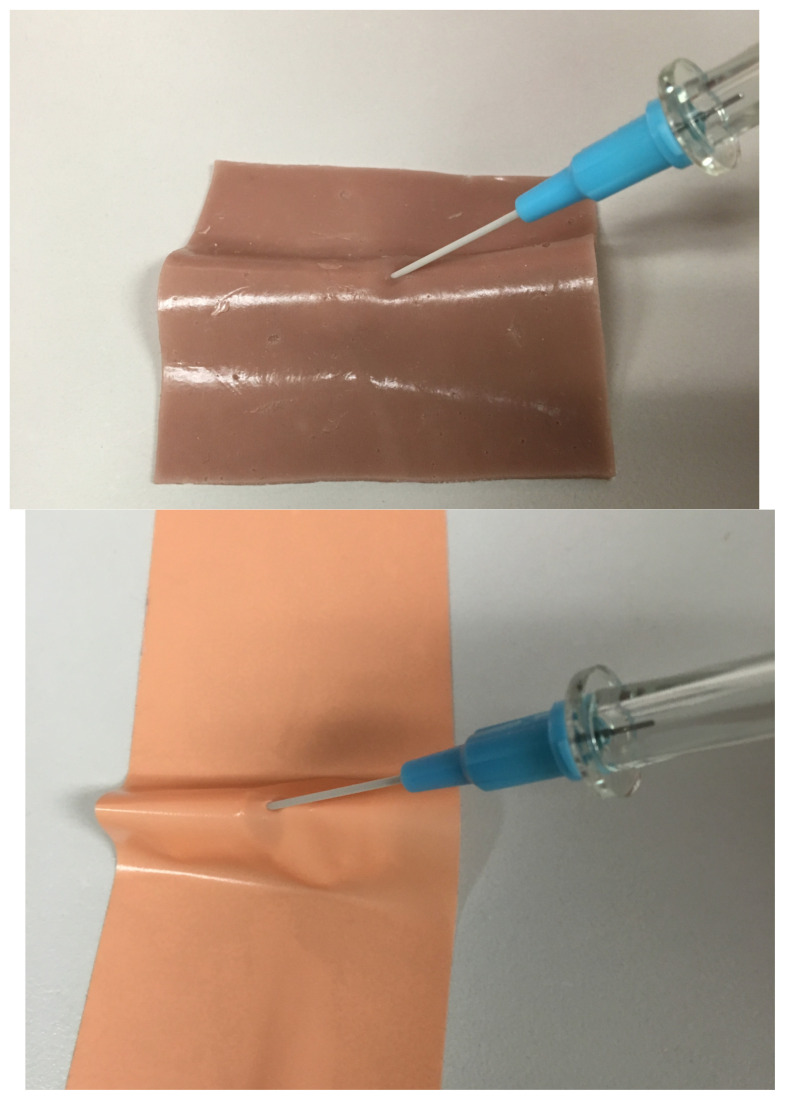
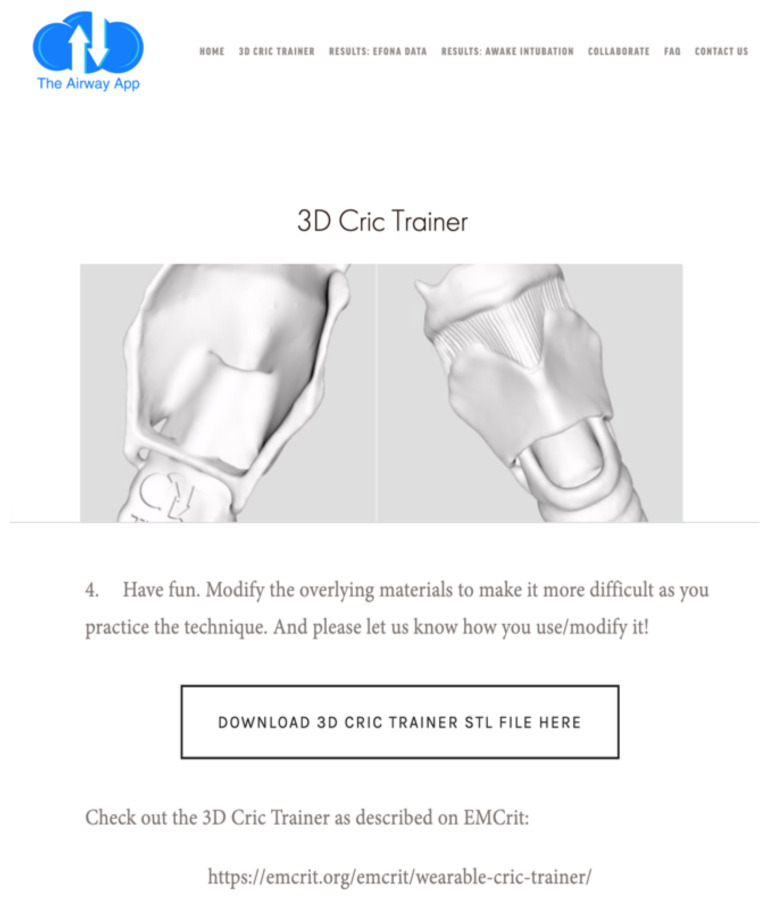
Trainers were created to enhance needle cricothyrotomy training in this rarely performed, yet critical procedure. It was felt that this procedure was only discussed in concept. There was no hands-on, procedure-based option available to realistically reproduce the procedure in a controlled training environment, and we felt the creation of a task trainer was ideal to address this deficiency. Once the trainers were created, we curated assigned pre-reading using a flipped classroom approach. The idea was to provide learners with multiple resources including textbook chapters, blogs, and podcasts, so that they could choose one or two resources that matched their learning style. We felt this was the best way to ensure learner retention. Additionally, we created a PowerPoint presentation to illustrate the stepwise procedure, required equipment, indications/contraindications, and ventilation aspect of the procedure, which can be reviewed with learners prior to performing the hands-on portion of the skills station.In order to create such a trainer, we worked in conjunction with the OhioHealth Simulation Department to obtain a 3D printer. Adult cricothyrotomy trainers were previously purchased from The Airway App, a company specializing in airway management education. The company also provides a standard template library (.STL) file that contains code for 3D printing cricothyrotomy trainers. Using this code, we made changes to the scale in order to create a smaller model that would resemble neonatal, school-aged, and adolescent patients (25%, 33%, and 50% of the original adult trainer, respectively). These scale models, particularly the neonatal model, were chosen based on the neonatal cadaveric measurements researched by Navasa, et al.7To prepare the trainer for use, sim skin and sim tape were used to cover and obscure the landmarks. Learners were given the materials previously discussed in preparation of the skills lab. Although all sizes of trainers were used by the learners, particularly attention was paid to the neonatal trainer. Emphasis was placed on the difficulty finding landmarks during this procedure. Instructors were available for the entirety of the skill station in order to answer questions and give direct feedback. Debriefing was performed at the end of the skills session.
Post-simulation surveys were completed by PGY 1-4 emergency medicine resident physicians assessing pre- and post-simulation procedural comfortability using a 5-point Likert scale. In this survey, 1 represented "not comfortable at all" while 5 represented "completely comfortable." Two, three, and four showed a gradual increase in comfortability, respectively. Median pre- and post-scores were calculated with interquartile ranges (IQR). A two-tailed Mann-Whitney U test was performed for statistical significance. Realism and future use were also surveyed.
Thirty-one emergency medicine resident physicians ranging from PGY1 to PGY4 completed the post-simulation survey. Median pre-simulation score was 2 (IQR 1-2.5) and post-simulation score was 4 (IQR 3-4). The two-tailed Mann-Whitney U test showed statistical significance at p<0.01. Ninety-seven percent of participants felt the trainers were realistic and 100% would recommend them for future simulation use.
Novel 3D printed needle cricothyrotomy trainers are a much-needed addition to emergency medicine procedural training. Specifically, we focus on the use of low-cost, high-fidelity trainers for educating emergency medicine resident physicians. By using a pre-templated .STL file, we were able to manipulate sizes and dimensions to create several simulation trainers for simulating needle cricothyrotomy. Our results show that these trainers are valuable to emergency medicine procedural training, increasing resident comfortability. Furthermore, participants feel this is realistic and would recommend this for future simulations. Given the relative ease and low-cost nature of these trainers, in addition to their proven benefit with residents, we hope that others will be able to use similar trainers to help develop needle cricothyrotomy skills at all levels of training.
Needle cricothyrotomy, pediatrics, difficult airway, 3D printing, education.
三维打印环甲膜切开术训练器旨在用于急诊医学各级培训,既用于技能习得,也用于防止技能萎缩。
长期以来,模拟一直为培训医疗人员掌握极少执行的操作提供了一种手段。例如,外科环甲膜切开术几乎一直仅通过低仿真模型在模拟环境中进行练习。这种培训似乎缺乏针对儿科人群的针式环甲膜切开术模拟。针式环甲膜切开术仍然是儿科患者在“无法插管、无法给氧”情况下临时气道管理的护理标准。为了解决这一教育缺陷,我们利用基于证据的尸体文献设计了一种三维打印儿科针式环甲膜切开术训练器,该文献展示了新生儿环甲膜尺寸。这些训练器将作为一种模拟工具,帮助急诊医学住院医师在可控环境中学习执行一种罕见且高风险的操作。
在本次教育课程结束时,参与者应能够:讨论儿科人群针式环甲膜切开术的适应症和禁忌症;组装完成针式环甲膜切开术所需的设备;描述并执行新生儿和儿科针式环甲膜切开术的步骤;讨论术后通气选择。
为加强这种极少执行但至关重要的针式环甲膜切开术训练而制作了训练器。人们认为该操作仅在概念上进行了讨论。在可控的训练环境中,没有实际操作的、基于程序的选项来逼真地重现该操作,我们认为创建一个任务训练器是解决这一缺陷的理想方法。训练器制作完成后,我们采用翻转课堂的方法精心挑选了指定的预读材料。其理念是为学习者提供多种资源,包括教科书章节、博客和播客,以便他们可以选择一两种符合自己学习风格的资源。我们认为这是确保学习者记忆的最佳方式。此外,我们制作了一个PowerPoint演示文稿,以说明该操作的逐步过程、所需设备、适应症/禁忌症以及通气方面的内容,可在学习者进行技能站的实际操作部分之前与他们一起回顾。为了制作这样一个训练器,我们与俄亥俄健康模拟部合作以获得一台三维打印机。成人环甲膜切开术训练器此前购自气道应用公司,该公司专门从事气道管理教育。该公司还提供一个标准模板库(.STL)文件,其中包含用于三维打印环甲膜切开术训练器的代码。利用此代码,我们对尺寸进行了调整,以创建一个更小的模型,该模型分别类似于新生儿、学龄儿童和青少年患者(分别为原始成人训练器的25%、33%和50%)。这些比例模型,特别是新生儿模型,是根据纳瓦萨等人研究的新生儿尸体测量数据选择的。为使训练器可供使用,使用模拟皮肤和模拟胶带覆盖并模糊标志点。为学习者提供了之前在技能实验室准备中讨论过的材料。尽管学习者使用了所有尺寸的训练器,但特别关注了新生儿训练器。在此操作过程中,重点强调了寻找标志点的困难。在整个技能站期间都有教员提供帮助,以便回答问题并给予直接反馈。在技能课程结束时进行了总结汇报。
由1 - 4年级急诊医学住院医师完成模拟后调查,使用5点李克特量表评估模拟前后的操作舒适度。在该调查中,1表示“完全不舒服”,而5表示“完全舒服”。2、3和4分别表示舒适度逐渐增加。计算中位数前后得分及四分位间距(IQR)。进行双尾曼 - 惠特尼U检验以确定统计学意义。还对逼真度和未来使用情况进行了调查。
31名从PGY1到PGY4的急诊医学住院医师完成了模拟后调查。模拟前中位数得分为2(IQR 1 - 2.5),模拟后中位数得分为4(IQR 3 - 4)。双尾曼 - 惠特尼U检验显示p<0.01时有统计学意义。97%的参与者认为训练器逼真,100%会推荐在未来模拟中使用。
新型三维打印针式环甲膜切开术训练器是急诊医学操作训练急需的补充。具体而言,我们专注于使用低成本、高保真的训练器来培训急诊医学住院医师。通过使用预模板化的.STL文件,我们能够操纵尺寸和维度来创建多个用于模拟针式环甲膜切开术的模拟训练器。我们的结果表明,这些训练器对急诊医学操作训练很有价值,提高了住院医师的舒适度。此外,参与者认为这很逼真,并会推荐在未来模拟中使用。鉴于这些训练器相对容易制作且成本低,除了已证明对住院医师有益外,我们希望其他人能够使用类似的训练器来帮助在各级培训中培养针式环甲膜切开术技能。
针式环甲膜切开术、儿科、困难气道、三维打印、教育。