Mastenbrook Joshua D, Hughes Neil C, Fales William D, Overton David T
Western Michigan University Homer Stryker M.D. School of Medicine, Department of Emergency Medicine, Kalamazoo, MI.
J Educ Teach Emerg Med. 2020 Apr 15;5(2):I9-I20. doi: 10.21980/J8MM1R. eCollection 2020 Apr.
This pulmonary edema intubation simulator is designed to instruct paramedics, medical students, emergency medicine residents, emergency medical services fellows, and attending physicians.
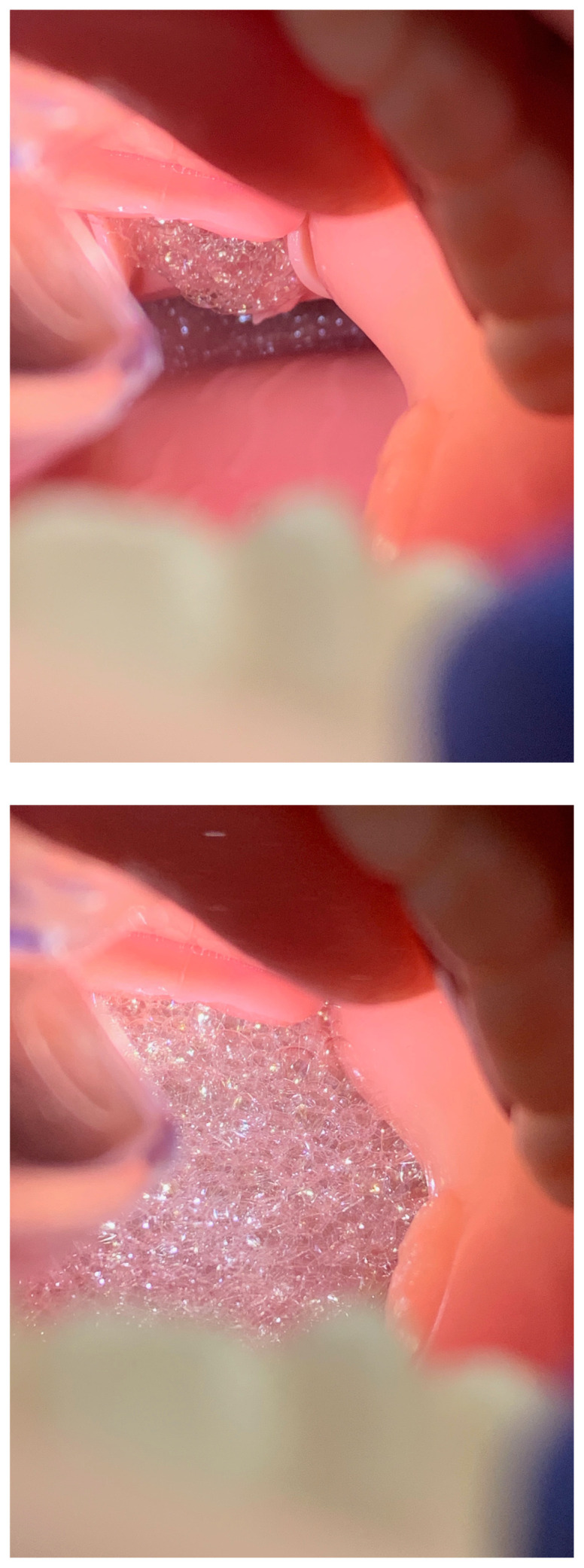
Acute pulmonary edema results in respiratory distress and may require endotracheal intubation. On occasion, pulmonary edema can result in copious amounts of pink, frothy sputum in the airway, complicating intubation by hindering the intubator's view. Although airway management skills are frequently taught in a simulation setting, the frothy sputum seen in acute pulmonary edema is not easily replicated. Several articles have been published in reference to simulation model development for difficult airway management due to emesis obscuring the view of the glottic opening.1,2 There is, however, a scarcity of literature describing pulmonary edema airway management simulator construction, with only one other model identified on our review of the literature, which utilized cadavers, baking soda, vinegar, and red food coloring.3In our simulation center, we teach a variety of learners who may be called upon to care for patients in acute pulmonary edema in their clinical practice, including medical students, residents from various specialties, practicing physicians and pre-hospital personnel. We wished to familiarize these trainees with the challenges associated with intubating patients with significant frothy secretions within the hypopharynx by developing a dynamic, realistic, portable and inexpensive model to simulate the airway manifestations associated with acute pulmonary edema.
By the end of the session, learners will be able to: 1. Discuss the pathophysiology of, and immediate stabilization management steps for, acute cardiogenic pulmonary edema. 2. List the indications, contraindications, and risks associated with intubating a patient with acute cardiogenic pulmonary edema. 3. Demonstrate effective communication and teamwork skills to manage the airway of a simulated patient in respiratory distress due to acute cardiogenic pulmonary edema. 4. Successfully and safely intubate a simulated patient with a difficult airway due to visual obstruction from frothy pulmonary edema secretions.
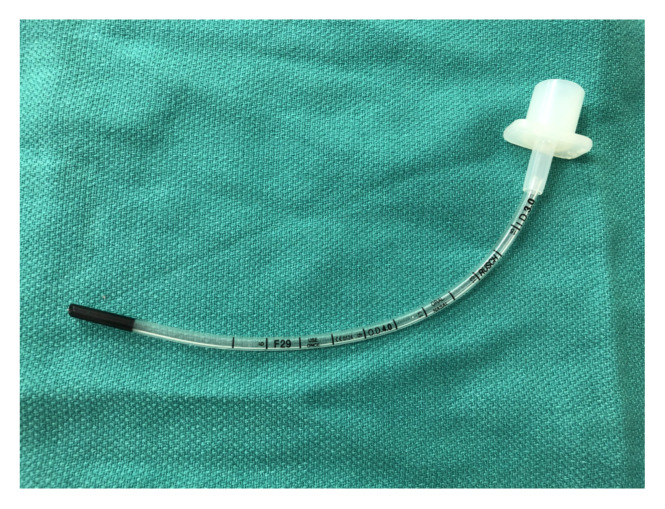
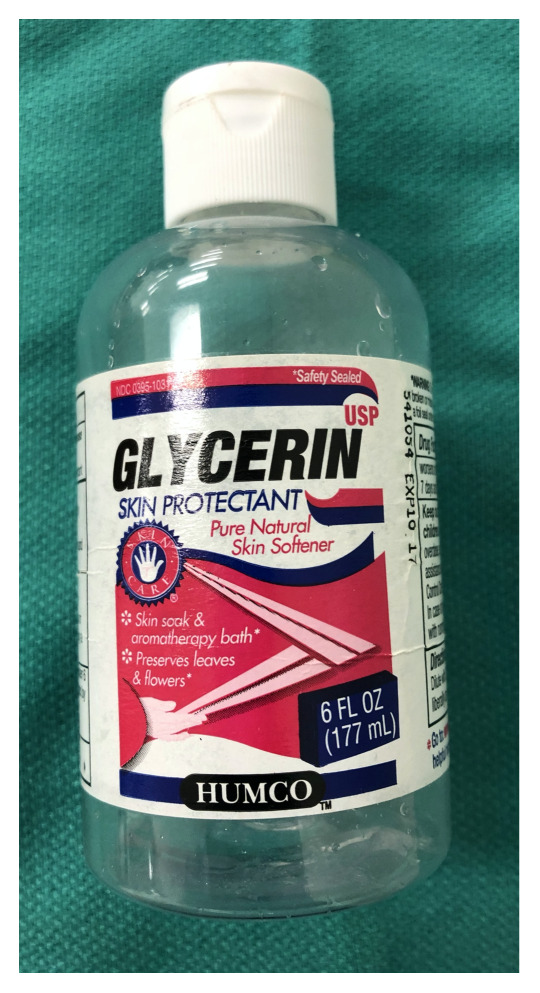
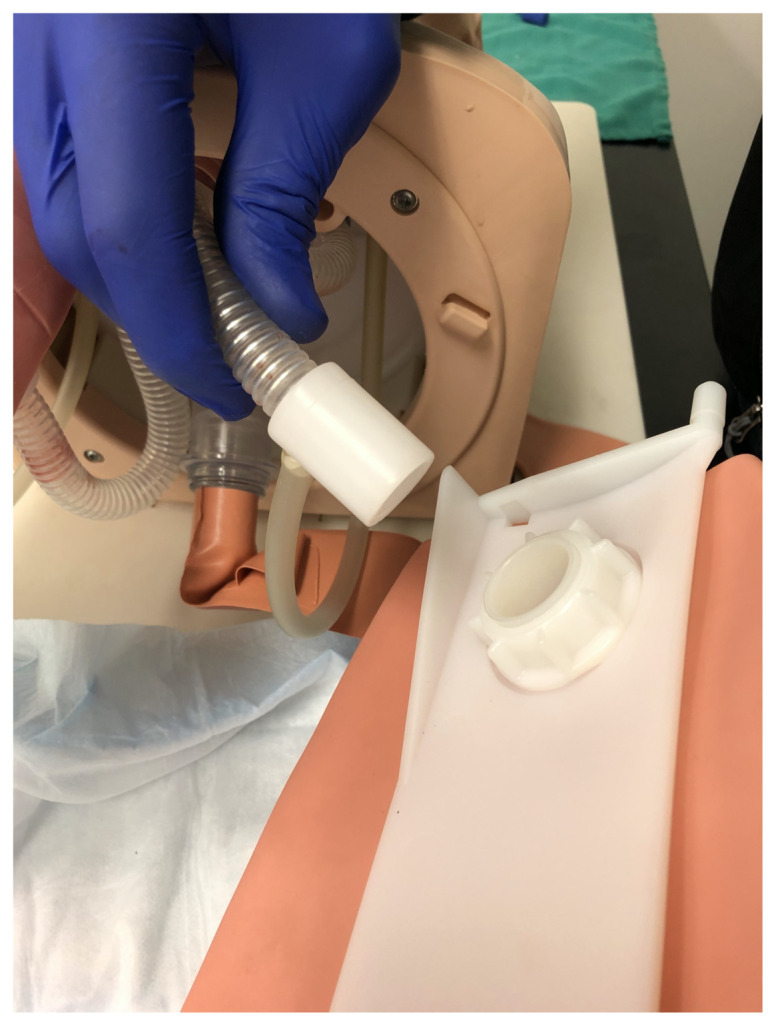
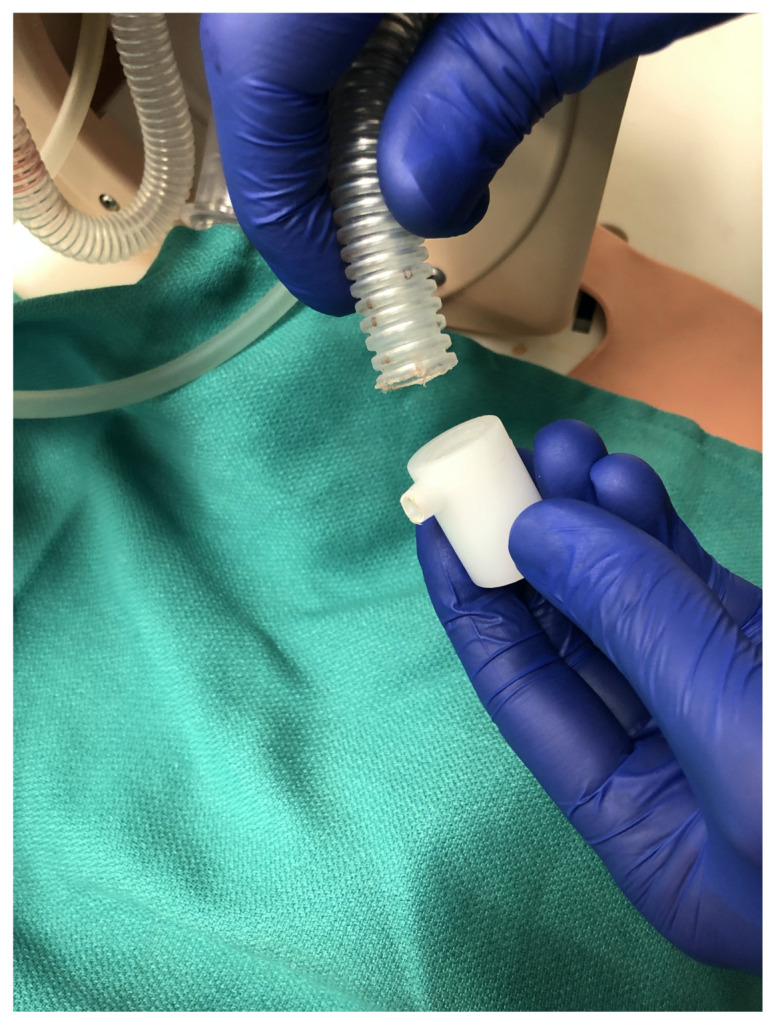
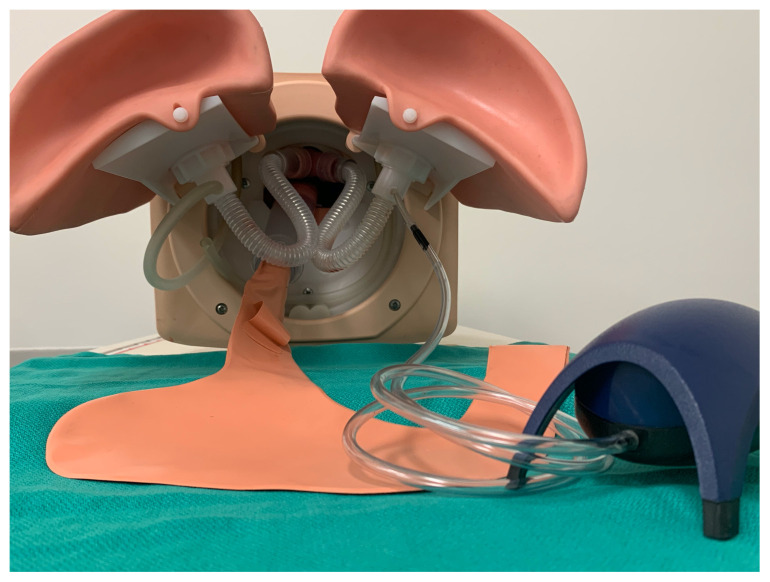
We adapted a previously owned commercial airway task trainer simulator using an aquarium pump, tubing, an air stone, and an endotracheal tube. Pulmonary edema solution was created with glycerin, dish soap, (distilled) water and simulated blood. The solution and air stone are placed in one of the simulator's lungs. Subsequently, turning on the aquarium air pump generates simulated pulmonary edema within the lung itself, which froths up and out of the trachea and into the hypopharynx, mimicking the gross pathophysiological process.Learners complete pre-reading assignments prior to attending a small group didactic-practical session. Following a brief case discussion, led by the instructor, about the management of a patient in respiratory distress due to acute pulmonary edema, learners transition to a hands-on experience intubating the pulmonary edema manikin with the use of direct and video laryngoscopy, aided by a large bore Yankauer for suction and a bougie. Depending on the training level of the learners, the instructor will use judgment and may elect to demonstrate intubating the manikin using video laryngoscopy before the learners attempt the procedure. The authors recommend that the instructor use video laryngoscopy for teaching purposes so that all learners can visualize the intubation techniques (Yankauer, bougie) in the context of copious pulmonary edema fluid obscuring the glottis and surrounding airway structures.The practical portion is dedicated solely to intubation, with one learner assuming the role of the intubator and another assuming the role of a respiratory therapist, while the other leaners observe and/or provide real-time feedback. Learners rotate through these aforementioned roles. To maintain efficiency of the simulation session and maximize the number of intubation attempts each learner receives, the session is designed to begin with a case discussion about the management of a patient with acute pulmonary edema up through the timepoint of successful intubation, followed by a practical portion where the learners perform multiple intubations on the innovative pulmonary edema airway management task trainer. During the practical portion, real-time constructive feedback is given to each learner. At the end of the simulation session, a debriefing is completed.This model can be used to address several ACGME Emergency Medicine Milestones,4 specifically Milestone 9 (General Approach to Procedures - PC9), Level 4 (Performs indicated procedures on any patients with challenging features [eg, poorly identifiable landmarks, at extremes of age or with comorbid conditions], and also Milestone 10 (Airway Management - PC10), Level 4 (Performs airway management in any circumstance taking steps to avoid potential complications). This model can also be used to address ACGME Emergency Medical Services Milestones,5 specifically "Procedures Performed in the Pre-hospital Environment - Patient Care," Level 4 (Performs indicated procedures on any patients, including those with challenging features (eg, poorly identifiable landmarks, at extremes of age or with co-morbid conditions).
At the conclusion of the session, verbal feedback is sought from each participant by the instructor: How helpful did you find this simulation experience for learning about airway management in patients with acute pulmonary edema? Did you find the pulmonary edema intubation model to be realistic? Following this simulation experience, how would you rate your personal confidence in terms of managing an airway complicated by acute pulmonary edema?
For under fifty dollars, we have been able to adapt one of our previously owned airway management task trainers to build a pulmonary edema intubation simulator. It has been used in a wide variety of settings for different learners, including medical students, residents, fellows and pre-hospital providers. Since the 2016-2017 academic year, two hundred and twenty-six emergency medicine residents (PGY1, PGY2, and PGY3) have successfully used our innovative pulmonary edema airway management task trainer. Qualitatively it has been well-received and felt to be realistic by both our learners and instructors based on verbal feedback received following the simulation sessions.
We are aware of only one prior report attempting to simulate the frothy sputum seen in acute pulmonary edema. Lipe, ., described mixing baking soda, vinegar and red food coloring in a cadaver hypopharynx just prior to an intubation attempt.3 This combination creates a fizzy frothy solution that fills the hypopharynx and pushes proximally into the mouth. This model is limited by design, however, in that it was unable to mimic a true in vivo appearance of a continuous flow of pulmonary edema-like fluid from the glottic opening. We feel we were able to overcome this limitation and also believe it is important for the leaner to experience the challenges of intubation when faced with copious secretions originating from within the lower airways. Our model generates the froth from within the lung itself, and it migrates proximally, similar to the dynamic pathophysiological process that occurs in vivo. Since we did not compare these two techniques, it is unknown which is more realistic. Neither the Lipe cadaver model nor our manikin model has been validated in terms of the realistic nature of the simulated pulmonary edema fluid. This would be ripe for future investigation. Nonetheless, informal qualitative feedback from our learners and instructors has been positive.Resident use of our innovative dynamic pulmonary edema airway management task trainer has been incorporated into our Emergency Medicine residency and Emergency Medical Services fellowship Clinical Competency Committee discussions with respect to ACGME Milestone satisfaction. Our model addresses level 4 of Emergency Medicine Milestone 9 (General Approach to Procedures) and Milestone 10 (Airway Management). Additionally, level 4 of Emergency Medical Services Milestone 2 (Procedures Performed in the Pre-hospital Environment - Patient Care) is addressed. Incorporating successful intubation of the dynamic pulmonary edema airway management task trainer has provided the EM and EMS faculty with a more objective measure by which to score the aforementioned milestones during the mid-year and year-end Clinical Competency Committee meetings.Overall, this innovation has met our objectives well. We have added this model to our library of more complicated airway management scenarios, such as vomitus and aspiration. Our emergency medicine residency program hosts a version of the difficult airway course and includes this pulmonary edema simulation station as part of that course. The model is very portable, allowing us to transport it to different sites for use. It is inexpensive, costing less than $50 to construct. Finally, the design is readily adaptable to any standard airway training manikin that has a simulated hollow lung with a detachable connection to a conduit representing a bronchus, which has a direct connection with a simulated trachea into which an endotracheal tube can physically be passed.
Airway management, difficult airway, intubation, obstructed airway, pulmonary edema, video laryngoscopy, visual obstruction.
这款肺水肿插管模拟器旨在培训护理人员、医学生、急诊医学住院医师、急诊医疗服务研究员以及主治医生。
急性肺水肿会导致呼吸窘迫,可能需要进行气管插管。有时,肺水肿会导致气道内出现大量粉红色泡沫痰,妨碍插管者的视野,使插管变得复杂。尽管气道管理技能通常在模拟环境中教授,但急性肺水肿中出现的泡沫痰并不容易复制。已有几篇文章发表,涉及因呕吐物遮挡声门开口视野而导致的困难气道管理模拟模型的开发。然而,描述肺水肿气道管理模拟器构建的文献却很匮乏,在我们的文献综述中仅发现另一个模型,该模型使用尸体、小苏打、醋和红色食用色素。在我们的模拟中心,我们培训各种可能在临床实践中照顾急性肺水肿患者的学习者,包括医学生、各专科住院医师、执业医生和院前急救人员。我们希望通过开发一个动态、逼真、便携且廉价的模型,使这些学员熟悉在存在大量下咽泡沫分泌物的情况下为患者插管所面临的挑战,以模拟与急性肺水肿相关的气道表现。
课程结束时,学习者将能够:1. 讨论急性心源性肺水肿的病理生理学以及立即稳定病情的管理步骤。2. 列出为急性心源性肺水肿患者插管的适应证、禁忌证和风险。3. 展示有效的沟通和团队协作技能,以管理因急性心源性肺水肿导致呼吸窘迫的模拟患者的气道。4. 成功且安全地为因泡沫状肺水肿分泌物导致视野受阻的困难气道模拟患者插管。
我们使用水族箱泵、管道、气石和气管导管对一台先前购置的商用气道任务训练模拟器进行了改装。用甘油、洗洁精、(蒸馏水)和模拟血液配制了肺水肿溶液。将溶液和气石放置在模拟器的一个肺中。随后,打开水族箱气泵,在肺内产生模拟的肺水肿,使其泡沫化并从气管涌出进入下咽,模拟总体病理生理过程。学习者在参加小组理论 - 实践课程之前完成预读作业。在教师引导下进行关于急性肺水肿导致呼吸窘迫患者管理的简短病例讨论后,学习者过渡到实际操作,使用直接喉镜和视频喉镜为肺水肿人体模型插管,并借助大口径扬卡厄吸引器和探条辅助。根据学习者的培训水平,教师将进行判断,并可能在学习者尝试操作之前选择使用视频喉镜演示为人体模型插管。作者建议教师使用视频喉镜进行教学,以便所有学习者能够在大量肺水肿液遮挡声门和周围气道结构的情况下可视化插管技术(扬卡厄吸引器、探条)。实际操作部分专门用于插管,一名学习者担任插管者,另一名学习者担任呼吸治疗师,其他学习者进行观察和/或提供实时反馈。学习者轮流扮演上述角色。为了保持模拟课程的效率并最大限度增加每个学习者的插管尝试次数,课程设计为先进行关于急性肺水肿患者管理直至成功插管时间点的病例讨论,然后是实际操作部分,学习者在创新的肺水肿气道管理任务训练器上进行多次插管。在实际操作过程中,会给每个学习者提供实时建设性反馈。模拟课程结束时,进行总结汇报。该模型可用于满足美国研究生医学教育认证委员会(ACGME)急诊医学的多个里程碑要求,特别是里程碑9(程序的一般方法 - PC9),第4级(对任何具有挑战性特征的患者进行指定程序[例如,难以识别的标志、年龄极端或患有合并症]),以及里程碑10(气道管理 - PC10),第4级(在任何情况下进行气道管理并采取措施避免潜在并发症)。该模型还可用于满足ACGME急诊医疗服务的里程碑要求,特别是“院前环境中执行的程序 - 患者护理”,第4级(对任何患者进行指定程序,包括那些具有挑战性特征的患者[例如,难以识别的标志、年龄极端或患有合并症])。
课程结束时,教师向每位参与者寻求口头反馈:您认为这种模拟体验对学习急性肺水肿患者的气道管理有多大帮助?您觉得肺水肿插管模型逼真吗?经历这次模拟体验后,您对管理因急性肺水肿而复杂的气道的个人信心如何评分?
花费不到五十美元,我们就能够对一台先前购置的气道管理任务训练器进行改装,构建一个肺水肿插管模拟器。它已在各种环境中用于不同的学习者,包括医学生、住院医师、研究员和院前急救人员。自2016 - 2017学年以来,226名急诊医学住院医师(PGY1、PGY2和PGY3)成功使用了我们创新的肺水肿气道管理任务训练器。根据模拟课程后收到的口头反馈,从定性角度来看,它受到了学习者和教师的好评,并且被认为很逼真。
我们知道之前只有一份报告试图模拟急性肺水肿中出现的泡沫痰。Lipe等人描述在插管尝试前在尸体下咽中混合小苏打、醋和红色食用色素。这种组合会产生一种冒泡的泡沫溶液,充满下咽并向口腔近端推进。然而,该模型在设计上存在局限性,即它无法模拟从声门开口持续流出的类似肺水肿液体的真实体内外观。我们认为我们能够克服这一局限性,并且还认为让学习者体验面对来自下呼吸道的大量分泌物时插管的挑战很重要。我们的模型从肺本身产生泡沫,并向近端迁移,类似于体内发生的动态病理生理过程。由于我们没有比较这两种技术,所以哪种更逼真尚不清楚。无论是Lipe的尸体模型还是我们的人体模型,在模拟肺水肿液的逼真程度方面都尚未得到验证。这将是未来研究的一个成熟领域。尽管如此,我们的学习者和教师的非正式定性反馈是积极的。住院医师使用我们创新的动态肺水肿气道管理任务训练器已被纳入我们急诊医学住院医师培训和急诊医疗服务研究员培训的临床能力委员会关于ACGME里程碑满意度的讨论中。我们的模型满足急诊医学里程碑9(程序的一般方法)和里程碑10(气道管理)的第4级要求。此外,还满足急诊医疗服务里程碑2(院前环境中执行的程序 - 患者护理)的第4级要求。将成功为动态肺水肿气道管理任务训练器插管纳入其中,为急诊医学(EM)和急诊医疗服务(EMS)教师在年中及年终临床能力委员会会议上对上述里程碑进行评分提供了更客观的标准。总体而言,这项创新很好地实现了我们的目标。我们已将此模型添加到我们更复杂的气道管理场景库中,如呕吐物和误吸场景。我们的急诊医学住院医师培训项目举办了一个困难气道课程版本,并将这个肺水肿模拟站作为该课程的一部分。该模型非常便携,使我们能够将其运输到不同地点使用。它价格低廉,构建成本不到50美元。最后,该设计很容易适应任何标准的气道训练人体模型,该模型具有模拟的中空肺,与代表支气管的导管有可拆卸连接,支气管与模拟气管直接相连,气管内可实际插入气管导管。
气道管理、困难气道、插管、气道阻塞、肺水肿、视频喉镜、视野受阻