Cai Wenying, Ruan Qianqian, Li Jiahao, Lin Li, Xi Liyan, Sun Jiufeng, Lu Sha
Department of Dermatology and Venereology, Sun Yat-sen Memorial Hospital of Sun Yat-Sen University, Guangzhou, People's Republic of China.
Guangdong Provincial Institute of Public Health, Guangzhou, People's Republic of China.
Infect Drug Resist. 2023 Jul 18;16:4687-4696. doi: 10.2147/IDR.S403863. eCollection 2023.
Deep fungal infection has become an important cause of infection and death in hospitalized patients, and this has worsened with increasing antifungal drug resistance.
A 3-year retrospective study was conducted to investigate the clinical characteristics, pathogen spectrum, and drug resistance of deep fungal infection in a regional hospital of Guangzhou, China.
Non-duplicate fungi isolates recovered from blood and other sterile body fluids of in-patients of the clinical department were identified using biochemical tests of pure culture with the API20C AUX and CHROMagar medium. Antifungal susceptibilities were determined by Sensititre YeastOne panel trays.
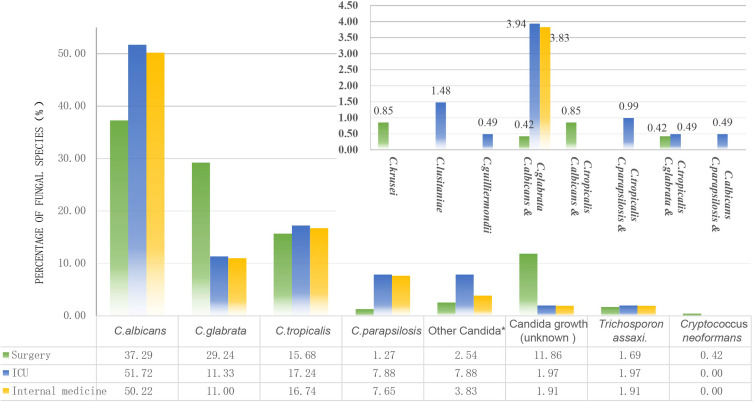
In this study, 525 patients (283 female, 242 male) with deep fungal infection were included, half of them were elderly patients (≥60 years) (54.67%, n=286). A total of 605 non-repetitive fungi were finally isolated from sterile samples, of which urine specimens accounted for 66.12% (n=400). Surgery, ICU, and internal medicine were the top three departments that fungi were frequently detected. The mainly isolated fungal species were (43.97%, n=266), (20.00%, n=121), and (17.02%, n=103), which contributed to over 80% of fungal infection. The susceptibility of the spp. to echinocandins, 5-fluorocytosine, and amphotericin B remained above 95%, while and to itraconazole were about 95%, and the dose-dependent susceptibility of to fluconazole was more than 90%. The echinocandins had no antifungal activity against in vitro (MIC>8 μg/mL), but azole drugs were good, especially voriconazole and itraconazole (MIC = 0.25 μg/mL).
The main causative agents of fungal infection were still the genus of . Echinocandins were the first choice for clinical therapy of infection, followed with 5-fluorocytosine and amphotericin B. Azole antifungal agents should be used with caution in and infections.
深部真菌感染已成为住院患者感染和死亡的重要原因,且随着抗真菌药物耐药性的增加,情况愈发严重。
进行一项为期3年的回顾性研究,以调查中国广州某地区医院深部真菌感染的临床特征、病原菌谱和耐药性。
采用API20C AUX和CHROMagar培养基对临床科室住院患者血液及其他无菌体液中分离出的非重复真菌菌株进行纯培养生化鉴定。采用Sensititre YeastOne平板试剂盒测定抗真菌药敏性。
本研究纳入525例深部真菌感染患者(女性283例,男性242例),其中一半为老年患者(≥60岁)(54.67%,n = 286)。最终从无菌样本中分离出605株非重复真菌,其中尿液标本占66.12%(n = 400)。外科、重症监护病房和内科是真菌检出率最高的三个科室。主要分离出的真菌种类为[具体真菌种类1](43.97%,n = 266)、[具体真菌种类2](20.00%,n = 121)和[具体真菌种类3](17.02%,n = 103),这三种真菌导致了超过80%的真菌感染。[具体真菌种类1]对棘白菌素、5-氟胞嘧啶和两性霉素B的敏感性仍高于95%,[具体真菌种类2]和[具体真菌种类3]对伊曲康唑的敏感性约为95%,[具体真菌种类3]对氟康唑的剂量依赖性敏感性超过90%。棘白菌素对[具体真菌种类4]在体外无抗真菌活性(MIC>8μg/mL),但唑类药物效果良好,尤其是伏立康唑和伊曲康唑(MIC = 0.25μg/mL)。
真菌感染的主要病原体仍是[具体真菌属]。棘白菌素是[具体真菌种类1]感染临床治疗的首选药物,其次是5-氟胞嘧啶和两性霉素B。在[具体真菌种类2]和[具体真菌种类3]感染中应谨慎使用唑类抗真菌药物。