Baylor Heart and Vascular Institute, Dallas, TX (M.P.).
Imperial College London, United Kingdom (M.P.).
Circulation. 2023 Jul 25;148(4):354-372. doi: 10.1161/CIRCULATIONAHA.123.064346. Epub 2023 Jul 24.
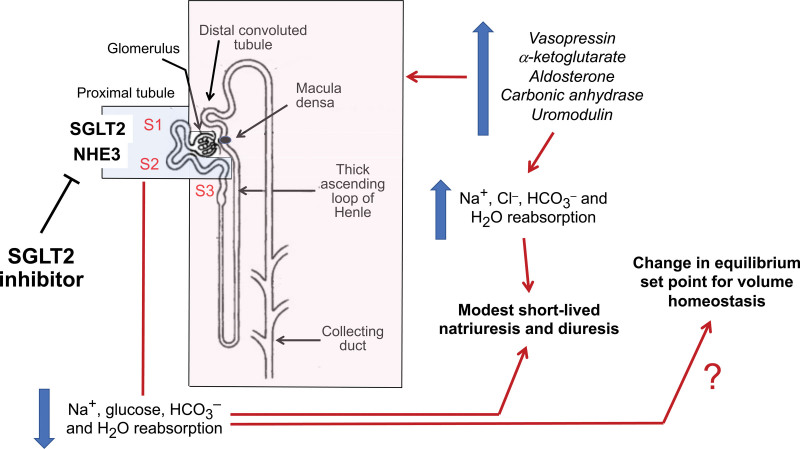
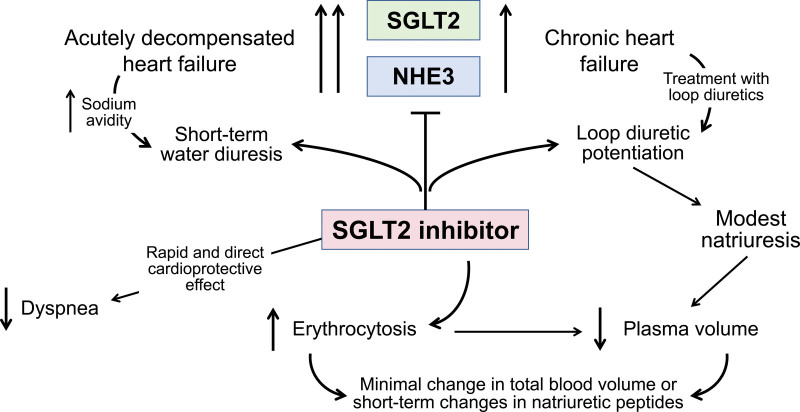
SGLT2 (sodium-glucose cotransporter 2) inhibitors interfere with the reabsorption of glucose and sodium in the early proximal renal tubule, but the magnitude and duration of any ensuing natriuretic or diuretic effect are the result of an interplay between the degree of upregulation of SGLT2 and sodium-hydrogen exchanger 3, the extent to which downstream compensatory tubular mechanisms are activated, and (potentially) the volume set point in individual patients. A comprehensive review and synthesis of available studies reveals several renal response patterns with substantial variation across studies and clinical settings. However, the common observation is an absence of a large acute or chronic diuresis or natriuresis with these agents, either when given alone or combined with other diuretics. This limited response results from the fact that renal compensation to these drugs is rapid and nearly complete within a few days or weeks, preventing progressive volume losses. Nevertheless, the finding that fractional excretion of glucose and lithium (the latter being a marker of proximal sodium reabsorption) persists during long-term treatment with SGLT2 inhibitors indicates that pharmacological tolerance to the effects of these drugs at the level of the proximal tubule does not meaningfully occur. This persistent proximal tubular effect of SGLT2 inhibitors can be hypothesized to produce a durable improvement in the internal set point for volume homeostasis, which may become clinically important during times of fluid expansion. However, it is difficult to know whether a treatment-related change in the volume set point actually occurs or contributes to the effect of these drugs to reduce the risk of major heart failure events. SGLT2 inhibitors exert cardioprotective effects by a direct effect on cardiomyocytes that is independent of the presence of or binding to SGLT2 or the actions of these drugs on the proximal renal tubule. Nevertheless, changes in the volume set point mediated by SGLT2 inhibitors might potentially act cooperatively with the direct favorable molecular and cellular effects of these drugs on cardiomyocytes to mediate their benefits on the development and clinical course of heart failure.
SGLT2(钠-葡萄糖协同转运蛋白 2)抑制剂干扰早期近端肾小管中葡萄糖和钠的重吸收,但随后的利钠或利尿作用的程度和持续时间是 SGLT2 上调的程度、下游补偿性管状机制激活的程度以及(潜在)个体患者的容量设定点之间相互作用的结果。对现有研究的全面回顾和综合揭示了几种肾脏反应模式,这些模式在研究和临床环境中存在很大差异。然而,共同的观察结果是,这些药物无论是单独使用还是与其他利尿剂联合使用,都不会引起大量急性或慢性利尿或利钠作用。这种有限的反应是由于肾脏对这些药物的代偿作用迅速且在几天或几周内几乎完全,从而防止了进行性的容量损失。尽管如此,在长期使用 SGLT2 抑制剂期间,葡萄糖和锂(后者是近端钠重吸收的标志物)的分数排泄仍然存在,这表明在近端小管水平上对这些药物的作用不存在药理学耐受性。SGLT2 抑制剂的这种持续的近端小管作用可以假设产生对体积内稳态的内部设定点的持久改善,这在液体扩张期间可能变得具有临床意义。然而,很难知道容量设定点的治疗相关变化是否实际发生或有助于这些药物降低主要心力衰竭事件的风险。SGLT2 抑制剂通过对心肌细胞的直接作用发挥心脏保护作用,而与 SGLT2 的存在或结合或这些药物对近端肾小管的作用无关。尽管如此,SGLT2 抑制剂介导的容量设定点变化可能与这些药物对心肌细胞的直接有利的分子和细胞作用协同作用,从而介导它们对心力衰竭的发展和临床过程的益处。