Department of Cardiology, Huazhong University of Science and Technology Union Shenzhen Hospital, Shenzhen, China.
Department of Cardiology, The First Affiliated Hospital of Jinan University, Guangzhou, China.
BMC Cardiovasc Disord. 2023 Jul 24;23(1):370. doi: 10.1186/s12872-023-03402-9.
The purpose of this meta-analysis is to evaluate the role of high-intensity statin pretreatment on coronary microvascular dysfunction in patients with coronary heart disease undergoing percutaneous coronary intervention (PCI).
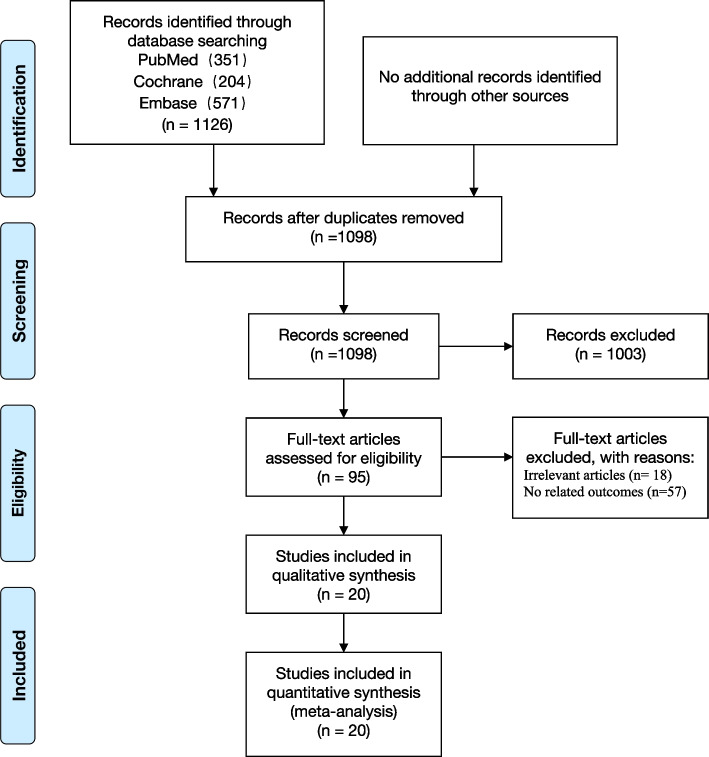
PubMed, Cochrane, and Embase were searched. This meta-analysis selection included randomized controlled trials (RCTs), involving high-intensity statin pretreatment as active treatment, and measurement of thrombolysis in myocardial infarction (TIMI), myocardial blush grade (MBG) or index of microvascular resistance (IMR) in coronary heart disease (CHD) patients undergoing PCI. I test was used to evaluate heterogeneity. Pooled effects of continuous variables were reported as Standard mean difference (SMD) and 95% confidence intervals (CI). Pooled effects of discontinuous variables were reported as risk ratios (RR) and 95% confidence intervals (CI). Random-effect or fix-effect meta-analyses were performed. The Benefit was further examined based on clinical characteristics including diagnosis and statin type by using subgroup analyses. Publication bias was examined by quantitative Egger's test and funnel plot. We performed sensitivity analyses to examine the robustness of pooled effects.
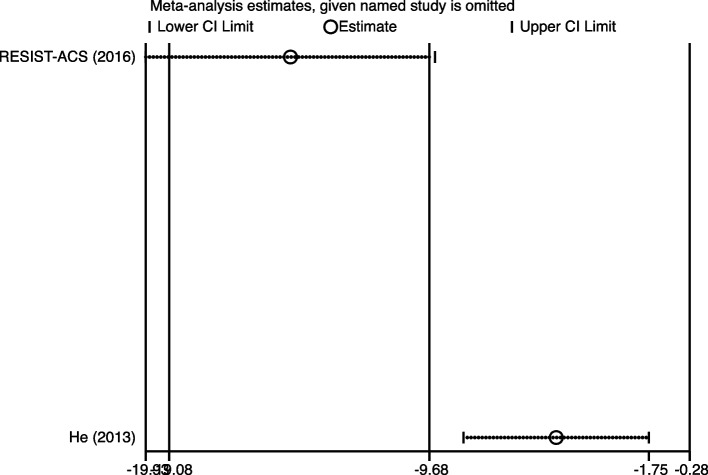
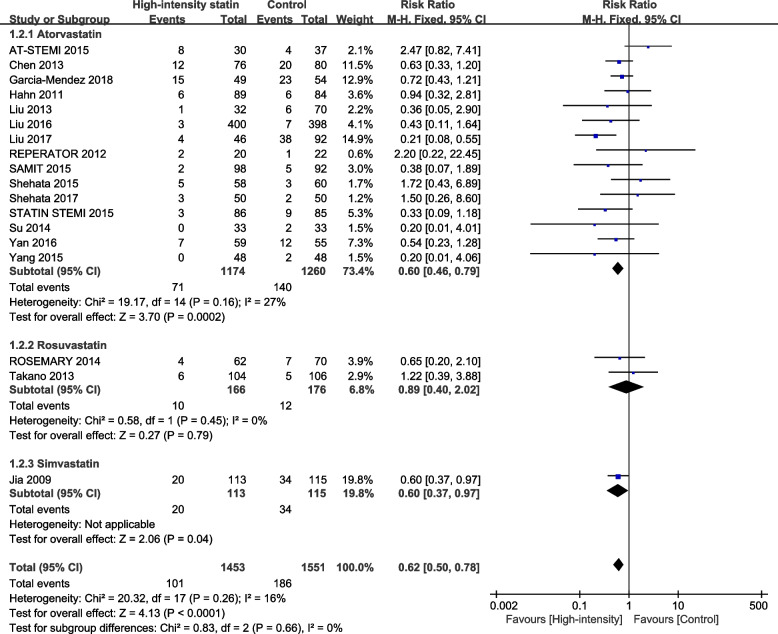
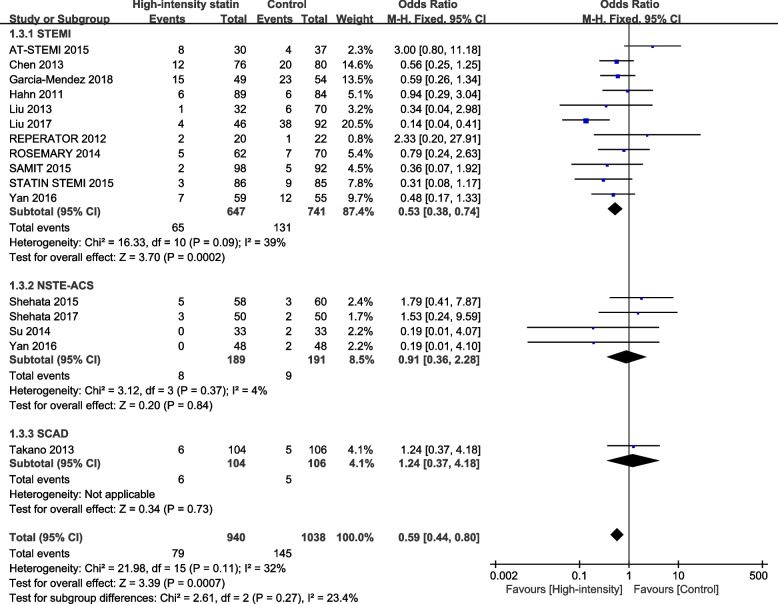
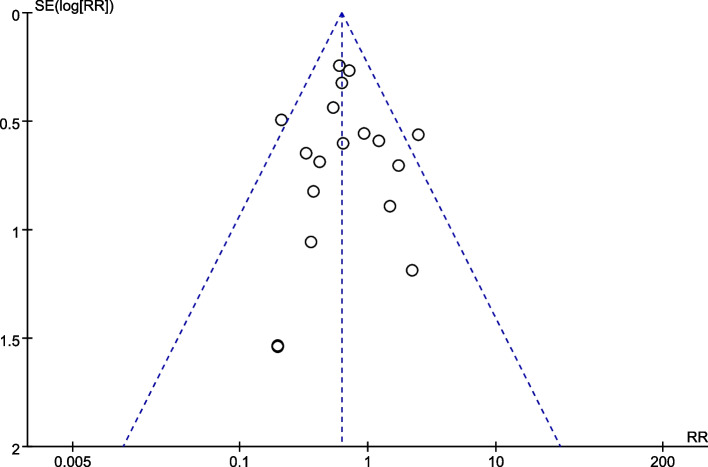
Twenty RCTs were enrolled. The data on TIMI < 3 was reported in 18 studies. Comparing with non-high-intensity statin, high-intensity statin pretreatment significantly improved TIMI after PCI (RR = 0.62, 95%CI: 0.50 to 0.78, P < 0.0001). The data on MBG < 2 was reported in 3 studies. The rate of MBG < 2 was not different between groups (RR = 1.29, 95% CI: 0.87 to 1.93, P = 0.21). The data on IMR was reported in 2 studies. High-dose statin pretreatment significantly improved IMR after PCI comparing with non-high-dose statin (SMD = -0.94, 95% CI: -1.47 to -0.42, P = 0.0004). There were no significant between-subgroup differences in subgroups based on statin type and diagnosis. Publication bias was not indicated by using quantitative Egger's test (P = 0.97) and funnel plot. Sensitivity analyses confirmed the robustness of these findings.
Comparing with non-high-intensity statin, high-intensity statin pretreatment significantly improved TIMI and IMR after PCI. In the future, RCTs with high quality and large samples are needed to test these endpoints.
本荟萃分析旨在评估高强度他汀预处理对接受经皮冠状动脉介入治疗(PCI)的冠心病患者冠状动脉微血管功能障碍的作用。
检索PubMed、Cochrane 和 Embase。本荟萃分析的选择包括随机对照试验(RCT),涉及高强度他汀预处理作为主动治疗,并测量接受 PCI 的冠心病(CHD)患者的心肌梗死溶栓治疗(TIMI)、心肌灌注分级(MBG)或微血管阻力指数(IMR)。使用 I² 检验评估异质性。连续变量的汇总效应以标准均数差(SMD)和 95%置信区间(CI)报告。不连续变量的汇总效应以风险比(RR)和 95%置信区间(CI)报告。进行随机效应或固定效应荟萃分析。进一步根据临床特征(包括诊断和他汀类型)进行亚组分析,以评估获益。使用定量 Egger 检验和漏斗图评估发表偏倚。我们进行敏感性分析以检查汇总效应的稳健性。
共纳入 20 项 RCT。18 项研究报告了 TIMI<3 的数据。与非高强度他汀相比,高强度他汀预处理可显著改善 PCI 后的 TIMI(RR=0.62,95%CI:0.50 至 0.78,P<0.0001)。3 项研究报告了 MBG<2 的数据。两组之间 MBG<2 的发生率无差异(RR=1.29,95%CI:0.87 至 1.93,P=0.21)。2 项研究报告了 IMR 的数据。与非高剂量他汀相比,高剂量他汀预处理可显著改善 PCI 后的 IMR(SMD=-0.94,95%CI:-1.47 至 -0.42,P=0.0004)。基于他汀类型和诊断的亚组分析未显示出组间有显著差异。使用定量 Egger 检验(P=0.97)和漏斗图未提示存在发表偏倚。敏感性分析证实了这些发现的稳健性。
与非高强度他汀相比,高强度他汀预处理可显著改善 PCI 后的 TIMI 和 IMR。未来需要高质量、大样本的 RCT 来检验这些终点。