Liu Jian, Wang Zizhuo, Wang Cheng, Zhang Yunong
School of Physical Education and Health, Heze University, Heze, Shandong, China.
Institute of Physical Education, Dongshin University, Naju, Jeollanam-do, Republic of Korea.
BMJ Open. 2025 May 30;15(5):e094309. doi: 10.1136/bmjopen-2024-094309.
To systematically evaluate the intervention effect of modified constraint-induced movement therapy (m-CIMT) on upper limb function in patients who had a stroke.
Systematic review and meta-analysis.
A computer-based search was conducted in PubMed, Cochrane Library, Embase, Web of Science and China National Knowledge Infrastructure for randomised controlled trials (RCTs) on the intervention effect of m-CIMT on upper limb function in patients who had a stroke, with the search conducted up until 23 May 2024.
We included only RCTs in which patients who had a stroke performed m-CIMT or m-CIMT in addition to the control group, and the outcome was upper limb function.
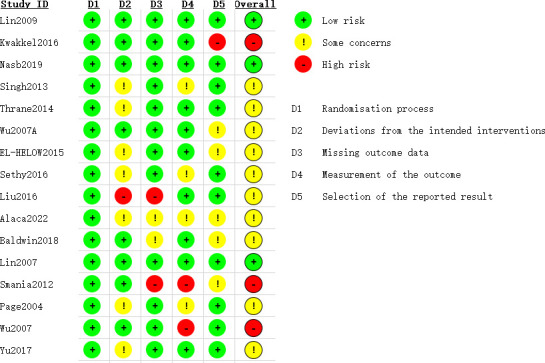
Data extraction and synthesis used the reporting checklist for systematic review based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. The risk of bias and methodological quality of included studies were evaluated by two independent investigators under the guidance of Cochrane risk of bias. Effect sizes were pooled, funnel plots were created and subgroup analyses were conducted using Stata V.17.0. If I²>50%, a random-effects model was applied; otherwise, a fixed-effects model was used. Publication bias was assessed through funnel plots and Egger's test. In the presence of publication bias, a trim-and-fill method was employed for further examination. The quality of evidence was evaluated using GRADEpro.
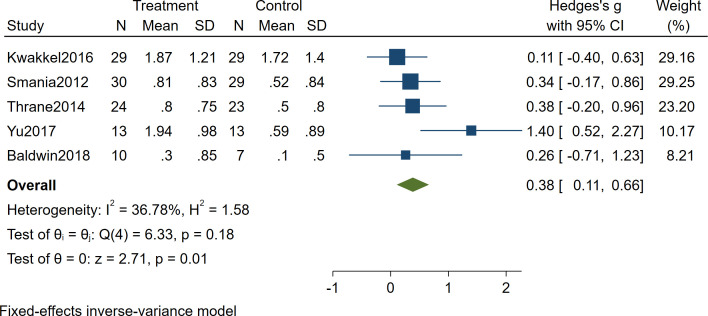
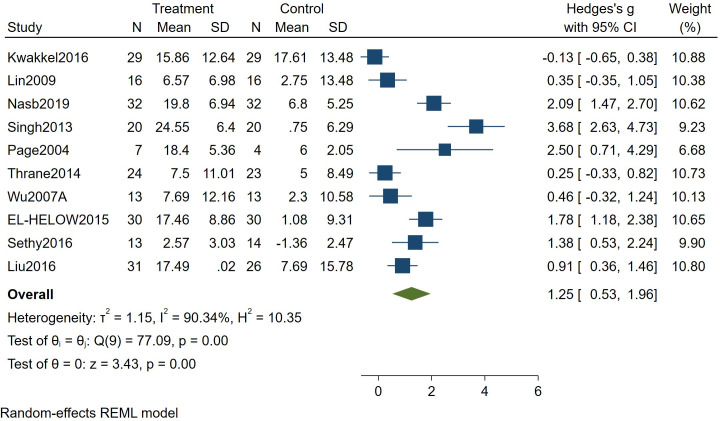
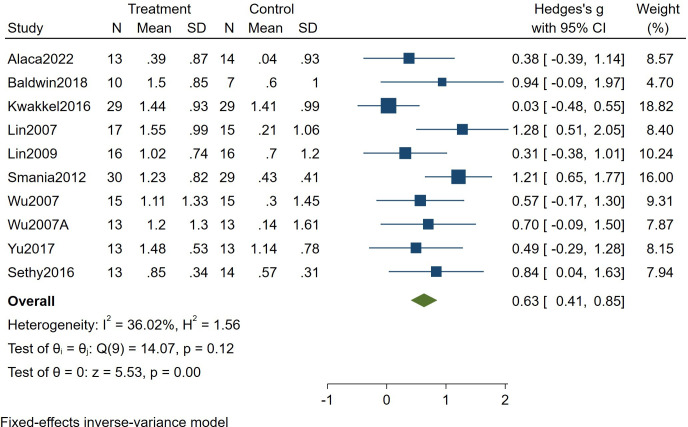
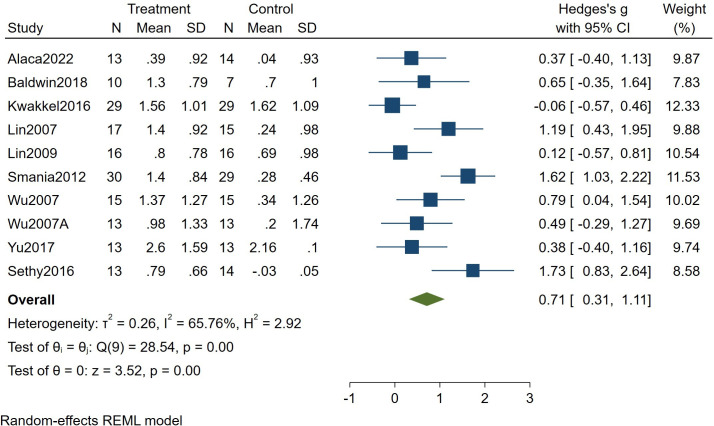
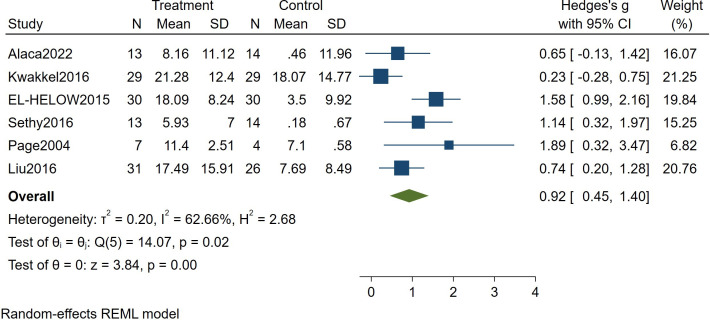
A total of 16 studies including 612 patients were included. Rehabilitation outcomes were assessed using the Fugl-Meyer Assessment (I²=90.34%), Motor Activity Log-Quality of Movement (I²=36.02%), Motor Activity Log-Amount of Use (I²=65.76%), Action Research Arm Test (I²=62.66%) and the Wolf Motor Function Test (I²=36.78%). Low-level evidence suggests that m-CIMT improves upper limb function in patients who had a stroke (all p<0.05). Subgroup analyses indicate that m-CIMT is effective in patients with 'chronic stroke' (p=0.001) and in patients who had a stroke with a course duration of '>2 months' (p=0.005). Intervention periods of '2-4 weeks' (p=0.008) and '5-12 weeks' (p<0.01), as well as intervention durations of '30-60 min' (p=0.006) and '120-180 min' (p=0.045), were all found to improve upper limb function in patients who had a stroke.
Low-level evidence suggests that m-CIMT can improve upper limb function in patients who had a stroke, although some indicators exhibit high heterogeneity. Therefore, this conclusion should be interpreted with caution. m-CIMT appears to improve upper limb function in patients who had a stroke with a course duration of more than 2 months, as well as in patients with chronic stroke. The intervention period should be at least 2 weeks, and each training session should last at least 30 min. Future studies should adopt more rigorous methodologies and larger sample sizes to further validate the efficacy of m-CIM.
CRD42024550028.
系统评价改良强制性运动疗法(m-CIMT)对脑卒中患者上肢功能的干预效果。
系统评价与荟萃分析。
通过计算机检索PubMed、Cochrane图书馆、Embase、科学网和中国知网,检索截至2024年5月23日关于m-CIMT对脑卒中患者上肢功能干预效果的随机对照试验(RCT)。
仅纳入脑卒中患者进行m-CIMT或除对照组外还进行m-CIMT且结局为上肢功能的RCT。
数据提取与合成采用基于系统评价和荟萃分析优先报告项目的系统评价报告清单。两名独立研究者在Cochrane偏倚风险指导下评估纳入研究的偏倚风险和方法学质量。使用Stata V.17.0合并效应量、绘制漏斗图并进行亚组分析。若I²>50%,则应用随机效应模型;否则,使用固定效应模型。通过漏斗图和Egger检验评估发表偏倚。若存在发表偏倚,则采用剪补法进行进一步检验。使用GRADEpro评估证据质量水平。
共纳入16项研究,包括612例患者。使用Fugl-Meyer评估法(I²=90.34%)、运动活动日志-运动质量(I²=36.02%)、运动活动日志-使用量(I²=65.76%)、动作研究上肢测试(I²=62.66%)和Wolf运动功能测试(I²=36.78%)评估康复结局。低质量证据表明,m-CIMT可改善脑卒中患者的上肢功能(所有p<0.05)。亚组分析表明,m-CIMT对“慢性脑卒中”患者(p=0.001)和病程“>2个月”的脑卒中患者有效(p=0.005)。“2-4周”(p=0.008)和“5-12周”(p<0.01)的干预期,以及“30-60分钟”(p=0.006)和“120-180分钟”(p=0.045)的干预时长均被发现可改善脑卒中患者的上肢功能。
低质量证据表明,m-CIMT可改善脑卒中患者的上肢功能,尽管部分指标存在高度异质性。因此,该结论应谨慎解读。m-CIMT似乎可改善病程超过2个月的脑卒中患者以及慢性脑卒中患者的上肢功能。干预期应至少为2周,每次训练时长应至少为30分钟。未来研究应采用更严谨的方法和更大的样本量,以进一步验证m-CIMT的疗效。
PROSPERO注册号:CRD42024550028。