Department of Thoracic Surgery, Tongji Medical College, The Central Hospital of Wuhan, Huazhong University of Science and Technology, Wuhan City, Hubei Province, China.
Department of Thoracic Surgery, Binzhou People's Hospital, Binzhou, China.
J Cardiothorac Surg. 2023 Jul 24;18(1):237. doi: 10.1186/s13019-023-02301-6.
This is a retrospective study of adverse events associated with preoperative computed tomography (CT)-guided hookwire or coil localisation. We analysed the experience and process flaws in resecting ground-glass nodules (GGNs) through video-assisted thoracoscopic surgery (VATS) and determined the remedial strategy.
Adverse events were evaluated in 40 patients with 45 GGNs who underwent CT-guided hookwire or coil localisation before VATS. For lesions not successfully marked or detected, palpation, resection of the highly suspected area, segmentectomy or lobectomy was performed.
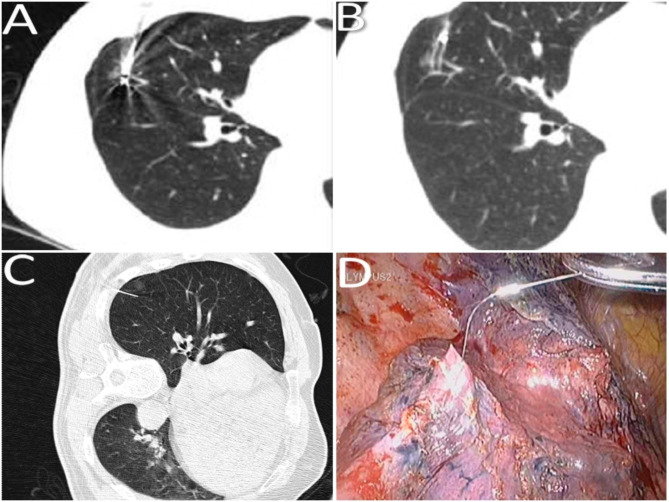
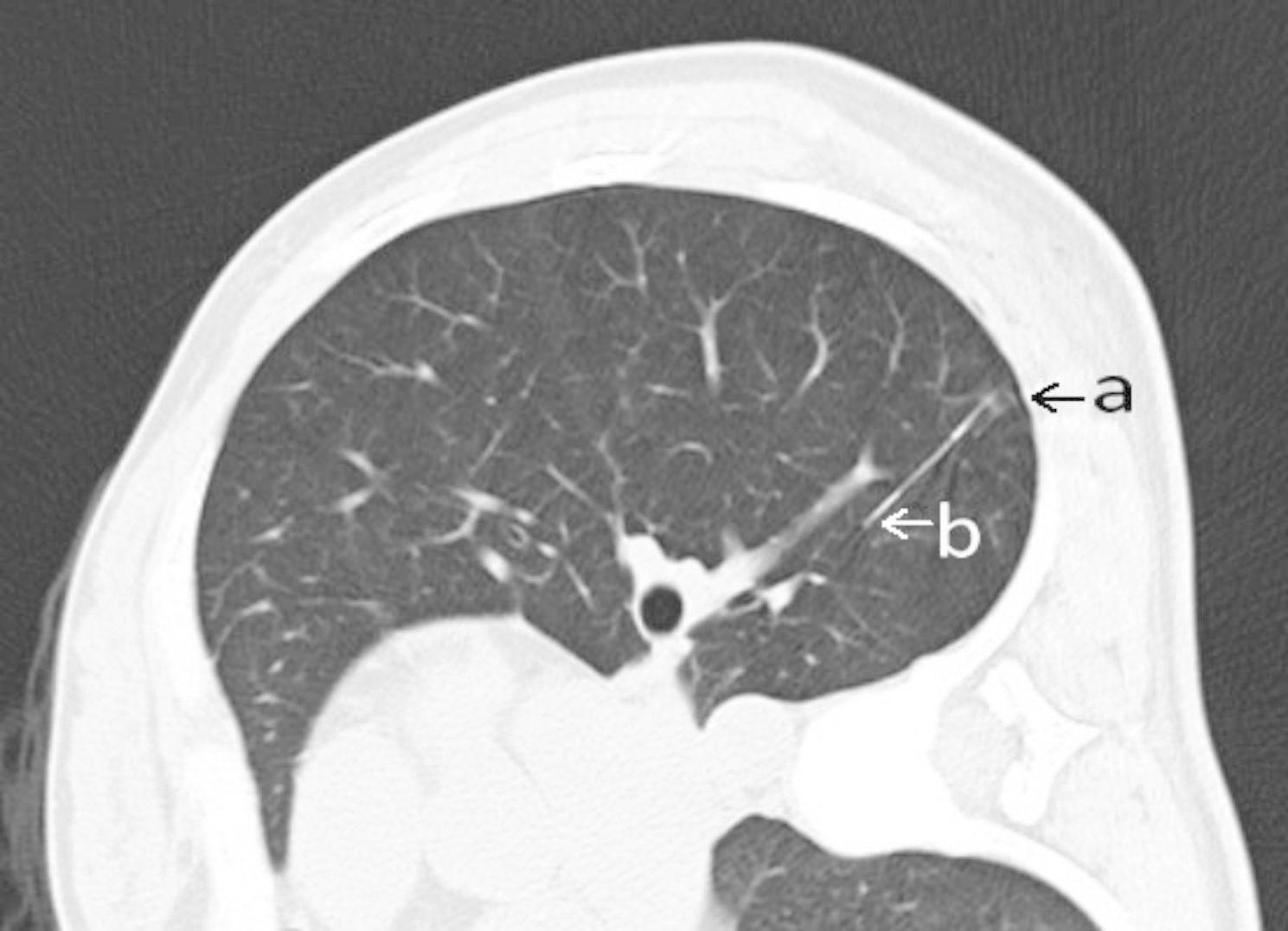
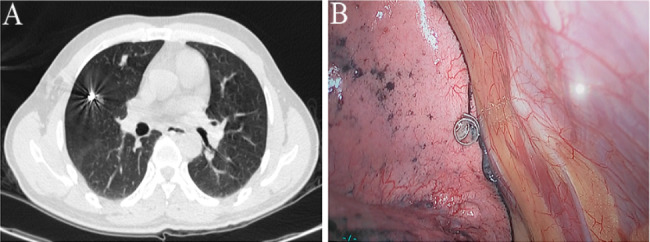
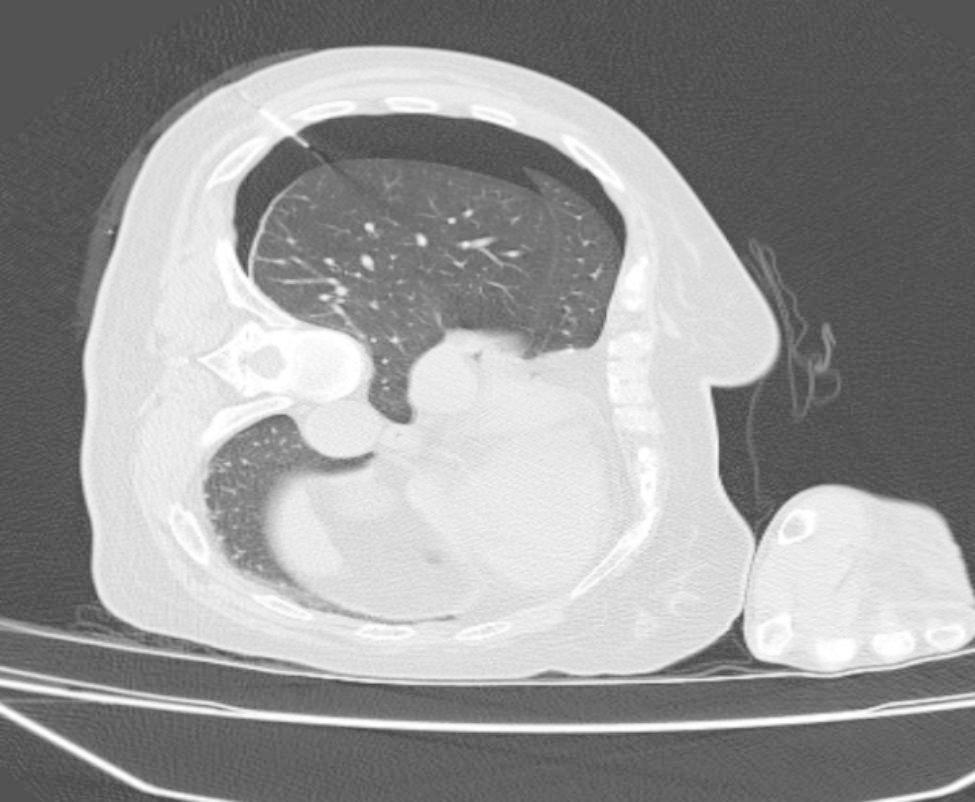
Among all adverse events, 15 were dislodgement of the marking materials, 5 were breakaway of the marking materials, 7 were > 2 cm distance between the lesions and the tips, 3 was marking material across the two adjacent lobes, 15 were pneumothorax and 2 were certain parts of marking materials stuck into the chest wall. All GGNs were resected successfully. 20 lesions were detected by palpation. 9 GGNs were discovered after the resection of highly suspected areas. Segmentectomies and lobectomies were performed directly on 7 and 9 GGNs, respectively.
When adverse events occur, a second intraoperative localisation, by resecting the highly suspected area either through non-anatomical resection (wedge resection) or anatomical resection (segmentectomy or lobectomy) using the VATS should be considered the alternatives for GGNs localization.
这是一项回顾性研究,旨在分析与术前计算机断层扫描(CT)引导下钩线或线圈定位相关的不良事件,并探讨通过电视辅助胸腔镜手术(VATS)切除磨玻璃结节(GGN)时的经验和流程缺陷,以及确定补救策略。
对 40 例 45 个 GGN 患者进行 CT 引导下钩线或线圈定位后,进行 VATS 手术。对于未成功标记或未发现的病灶,采用触诊、可疑区域切除、节段切除术或肺叶切除术。
所有不良事件中,标记材料移位 15 例,标记材料脱落 5 例,病灶与尖端之间的距离>2cm 7 例,标记材料穿过两个相邻肺叶 3 例,气胸 15 例,部分标记材料嵌入胸壁 2 例。所有 GGN 均成功切除。触诊发现 20 个病灶。切除可疑区域后发现 9 个 GGN。7 个 GGN 直接行节段切除术,9 个 GGN 直接行肺叶切除术。
当发生不良事件时,可考虑通过非解剖性切除(楔形切除术)或解剖性切除(节段切除术或肺叶切除术),用 VATS 再次进行术中定位,作为 GGN 定位的替代方法。