Department of Medicine, Brigham and Women's Hospital, Boston, Massachusetts, USA.
Vrije Universiteit Amsterdam, Amsterdam, Netherlands.
BMJ Open Qual. 2023 Jul;12(3). doi: 10.1136/bmjoq-2023-002271.
To reduce spending and improve quality, some primary care clinics in the USA have focused on high-need, high-cost (HNHC) Medicare beneficiaries, which include clinically distinct subpopulations: older adults with frailty, adults under 65 years with disability and beneficiaries with major complex chronic conditions. Nationally, the extent to which primary care clinics are high-performing 'Bright Spots'-clinics that achieve favourable outcomes at lower costs across HNHC beneficiary subpopulations-is not known.
To determine the prevalence of primary care clinics that perform highly on commonly used cost or quality measures for HNHC subpopulations.
Cross-sectional study using Medicare claims data from 2014 to 2015.
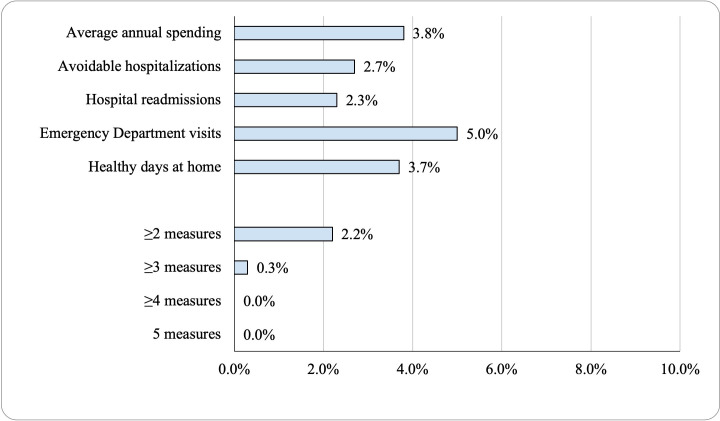
Annual spending, avoidable hospitalisations for ambulatory care-sensitive conditions, treat-and-release emergency department visits, all-cause 30-day unplanned hospital readmission rates and healthy days at home. Clinics were high performing when they ranked in the top quartile of performance for ≥4 measures for an HNHC subpopulation. 'Bright Spot' clinics were in the top quartile of performance for ≥4 measures across all the HNHC subpopulations.
A total of 2770 primary care clinics cared for at least 10 beneficiaries from each of the three HNHC subpopulations (adults under 65 with disability, older adults with frailty and beneficiaries with major complex chronic conditions). Less than 4% of clinics were high performing for each HNHC subpopulation; <0.5% of clinics were in the top quartile for all five measures for a given subpopulation. No clinics met the definition of a primary care 'Bright Spot'.
High-performing primary care clinics that achieved favourable health outcomes or lower costs across subpopulations of HNHC beneficiaries in the Medicare programme in 2015 were rare. Efforts are needed to support primary care clinics in providing optimal care to HNHC subpopulations.
为了降低成本并提高质量,美国的一些初级保健诊所专注于高需求、高费用(HNHC)的医疗保险受益人,其中包括临床特征明显的亚人群:体弱的老年人、65 岁以下有残疾的成年人以及患有主要复杂慢性疾病的受益人。在全国范围内,初级保健诊所作为绩效较高的“亮点”诊所的程度尚不清楚,这些诊所能够在所有 HNHC 受益人群中以较低的成本实现有利的结果。
确定在 HNHC 亚人群的常用成本或质量指标方面表现出色的初级保健诊所的比例。
使用 2014 年至 2015 年的医疗保险索赔数据进行的横断面研究。
每年的支出、可避免的门诊治疗敏感条件下的住院治疗、治疗后即释放的急诊科就诊、所有原因的 30 天非计划性住院再入院率和在家中的健康天数。当诊所的表现至少在 HNHC 亚人群的 4 项措施中排名前四分之一时,被认为是表现出色的。“亮点”诊所的表现在前四分之一,在所有 HNHC 亚人群的 4 项措施中均表现出色。
共有 2770 家初级保健诊所为每个 HNHC 亚人群(65 岁以下有残疾的成年人、体弱的老年人和患有主要复杂慢性疾病的受益人)至少治疗了 10 名受益人。不到 4%的诊所对每个 HNHC 亚人群都表现出色;<0.5%的诊所对特定亚人群的所有 5 项措施都处于前四分之一。没有诊所符合初级保健“亮点”的定义。
在 2015 年,医疗保险计划中 HNHC 受益人群的亚人群中,能够实现有利健康结果或降低成本的表现出色的初级保健诊所很少。需要努力支持初级保健诊所为 HNHC 亚人群提供最佳护理。