Singh Anshuman, Choudhary Anupam, Pai Vivek, Viswanath Kasi, K R Surag, Abhishek Goli V, Chawla Arun, Hegde Padmaraj
Urology, Kasturba Medical College of Manipal, Manipal Academy of Higher Education, Manipal, IND.
Cureus. 2023 Jun 23;15(6):e40879. doi: 10.7759/cureus.40879. eCollection 2023 Jun.
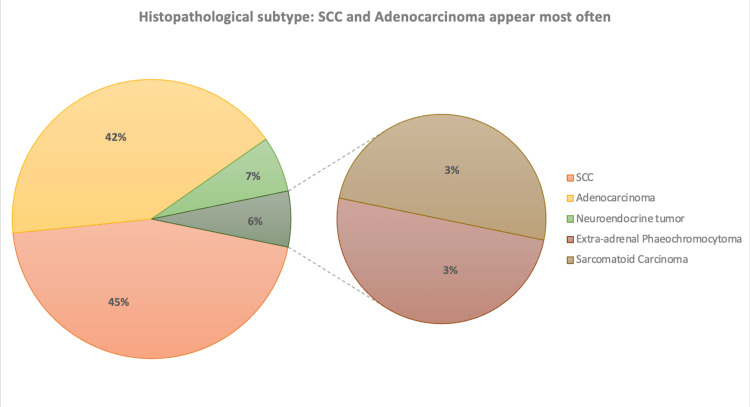
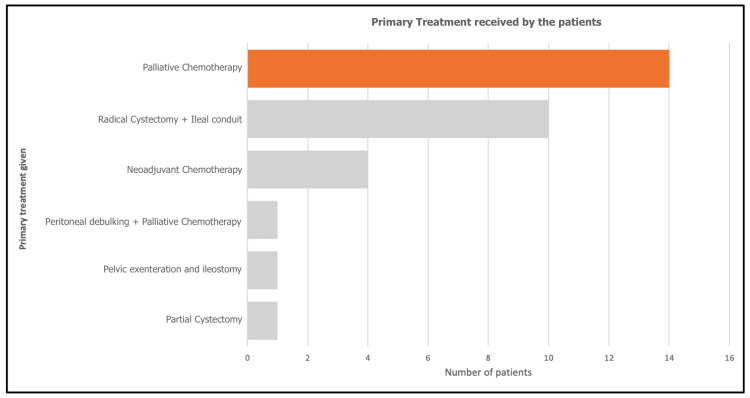
Introduction Non-transitional cell carcinomas of the bladder (NTCCB) represent a significant clinical challenge due to their rarity, heterogeneity, and poor prognosis. Despite their poor prognosis, the treatment of NTCCB has historically been based on the same principles used for transitional cell carcinomas (TCCs). Our study focuses on the management of non-transitional cell carcinomas and aims to identify areas where treatment outcomes can be improved based on our institutional experience. Materials and methods A retrospective analysis of patients with NTCCB who presented at Kasturba Hospital Manipal was conducted between 2012 to 2021. Patient data were collected, and demographic characteristics, presenting symptoms, history of other primary malignancies, comorbidities, location of the tumour, stage at presentation, histopathological subtype, site of systemic metastasis, and primary treatment given were analyzed descriptively. Median overall survival was determined by calculating the time from the initial diagnosis to the date of death. Results Among 31 patients with NTCCB, 15 (48%) presented with metastatic disease, five (16%) with locally advanced disease, and 11 (36%) with localized disease. The most common histopathological subtypes were squamous cell carcinoma and adenocarcinoma, as noted in 14 (45.2%) and 13 (41.9%) patients, respectively, followed by neuroendocrine tumours in two (6.5%), extra-adrenal phaeochromocytoma in one (3.3%), and sarcomatoid carcinoma in one (3.3%) patient, respectively. The lung was the most frequent site of systemic metastasis as noted in six (40%) patients, followed by the liver and skeletal system in three (20%) patients each, peritoneum in two (13.3%), cerebral cortex in one (6.7%), and non-regional lymph nodes in one (6.7%) patient. The primary treatment given included palliative chemotherapy in 14 (45.2%) patients, radical cystectomy with ileal conduit in 10 (32.3%), neoadjuvant chemotherapy only in four (12.9%), partial cystectomy in one (3.2%), pelvic exenteration with ileal conduit in one (3.2%), and peritoneal debulking with palliative chemotherapy in one (3.2%) patient. The overall median survival was 15 months, with a one-year survival rate of 67.4%. Conclusion NTCCB exhibits aggressive clinical behaviour and presents with nonspecific clinical features in the early stages, often leading to late diagnosis and an advanced tumour stage at presentation. Multi-institutional studies with larger patient cohorts are needed to recommend best clinical practices for early detection and optimal treatment strategies to improve patient survival.
引言
膀胱非移行细胞癌(NTCCB)因其罕见性、异质性和预后不良而构成重大的临床挑战。尽管其预后较差,但NTCCB的治疗在历史上一直基于用于移行细胞癌(TCC)的相同原则。我们的研究聚焦于非移行细胞癌的管理,并旨在根据我们机构的经验确定可改善治疗结果的领域。
材料与方法
对2012年至2021年期间在马尼帕尔卡斯图尔巴医院就诊的NTCCB患者进行回顾性分析。收集患者数据,并对人口统计学特征、临床表现、其他原发性恶性肿瘤病史、合并症、肿瘤位置、就诊时分期、组织病理学亚型、全身转移部位以及所给予的初始治疗进行描述性分析。通过计算从初始诊断到死亡日期的时间来确定中位总生存期。
结果
在31例NTCCB患者中,15例(48%)表现为转移性疾病,5例(16%)为局部晚期疾病,11例(36%)为局限性疾病。最常见的组织病理学亚型是鳞状细胞癌和腺癌,分别见于14例(45.2%)和13例(41.9%)患者,其次是神经内分泌肿瘤2例(6.5%)、肾上腺外嗜铬细胞瘤1例(3.3%)、肉瘤样癌1例(3.3%)。肺是最常见的全身转移部位,见于6例(40%)患者,其次是肝脏和骨骼系统各3例(20%)、腹膜2例(13.3%)、大脑皮质1例(6.7%)、非区域淋巴结1例(6.7%)。所给予的初始治疗包括14例(45.2%)患者接受姑息化疗、10例(32.3%)患者接受根治性膀胱切除术加回肠膀胱术、仅4例(12.9%)患者接受新辅助化疗、1例(3.2%)患者接受部分膀胱切除术、1例(3.2%)患者接受盆腔脏器清除术加回肠膀胱术、1例(3.2%)患者接受腹膜减瘤术加姑息化疗。总体中位生存期为15个月,一年生存率为67.4%。
结论
NTCCB表现出侵袭性的临床行为,早期具有非特异性临床特征,常导致诊断延迟和就诊时肿瘤分期较晚。需要开展涉及更大患者队列的多机构研究,以推荐早期检测的最佳临床实践和优化治疗策略,从而提高患者生存率。