Department of Metabolism, Digestion and Reproduction and Department of Surgery and Cancer, Institute of Reproductive and Developmental Biology, Faculty of Medicine, Imperial College London, Hammersmith Hospital campus, London, W12 0HS, UK.
Queen Charlotte's and Chelsea - Hammersmith Hospital, Imperial College Healthcare NHS Trust, London, UK.
BMC Med. 2023 Jul 27;21(1):274. doi: 10.1186/s12916-023-02965-w.
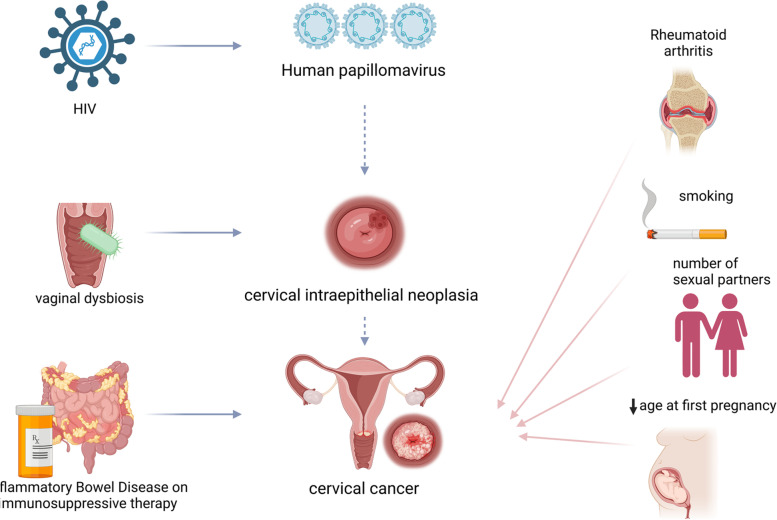
Persistent infection by oncogenic human papillomavirus (HPV) is necessary although not sufficient for development of cervical cancer. Behavioural, environmental, or comorbid exposures may promote or protect against malignant transformation. Randomised evidence is limited and the validity of observational studies describing these associations remains unclear.
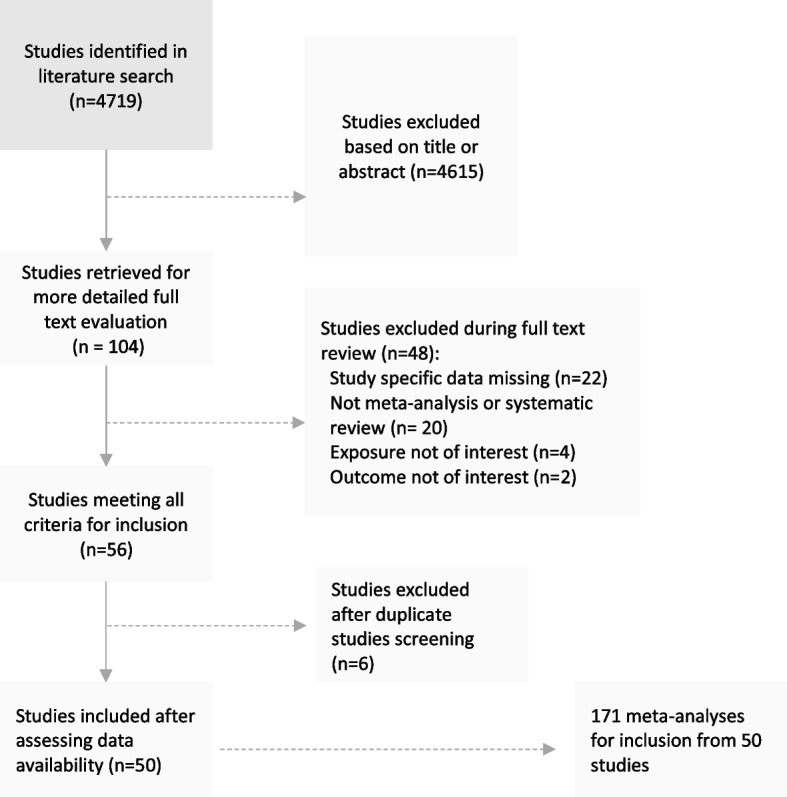
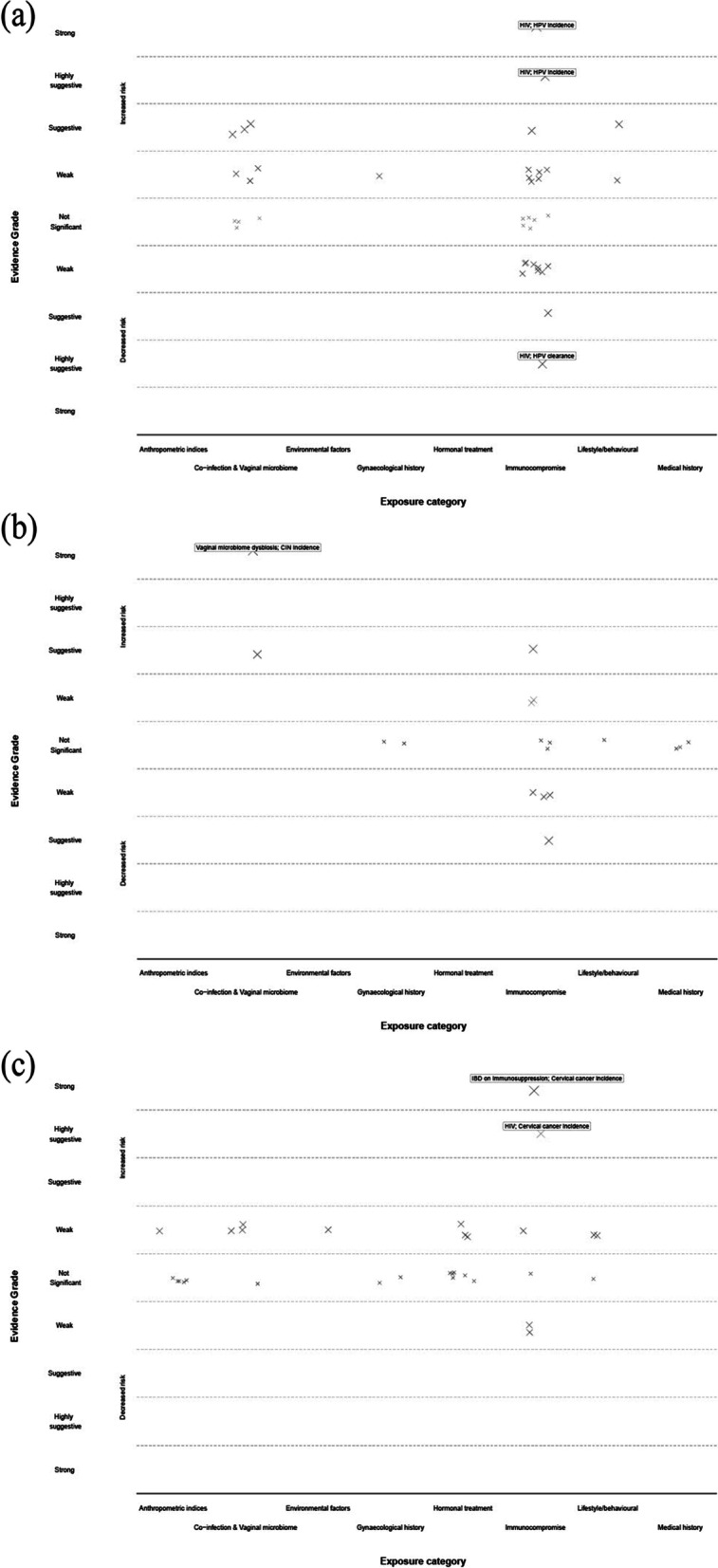
In this umbrella review, we searched electronic databases to identify meta-analyses of observational studies that evaluated risk or protective factors and the incidence of HPV infection, cervical intra-epithelial neoplasia (CIN), cervical cancer incidence and mortality. Following re-analysis, evidence was classified and graded based on a pre-defined set of statistical criteria. Quality was assessed with AMSTAR-2. For all associations graded as weak evidence or above, with available genetic instruments, we also performed Mendelian randomisation to examine the potential causal effect of modifiable exposures with risk of cervical cancer. The protocol for this study was registered on PROSPERO (CRD42020189995).
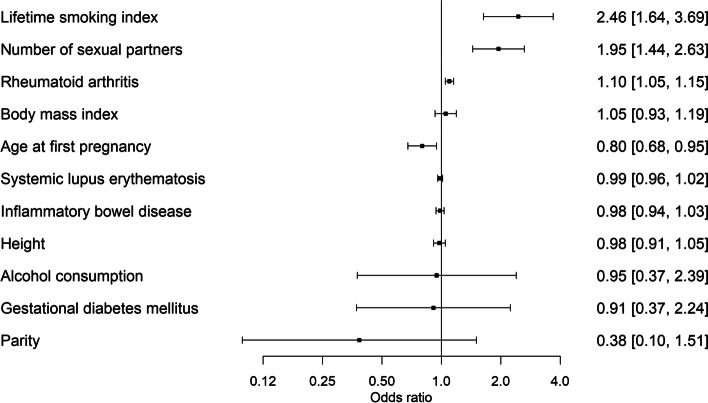
We included 171 meta-analyses of different exposure contrasts from 50 studies. Systemic immunosuppression including HIV infection (RR = 2.20 (95% CI = 1.89-2.54)) and immunosuppressive medications for inflammatory bowel disease (RR = 1.33 (95% CI = 1.27-1.39)), as well as an altered vaginal microbiome (RR = 1.59 (95% CI = 1.40-1.81)), were supported by strong and highly suggestive evidence for an association with HPV persistence, CIN or cervical cancer. Smoking, number of sexual partners and young age at first pregnancy were supported by highly suggestive evidence and confirmed by Mendelian randomisation.
Our main analysis supported the association of systemic (HIV infection, immunosuppressive medications) and local immunosuppression (altered vaginal microbiota) with increased risk for worse HPV and cervical disease outcomes. Mendelian randomisation confirmed the link for genetically predicted lifetime smoking index, and young age at first pregnancy with cervical cancer, highlighting also that observational evidence can hide different inherent biases. This evidence strengthens the need for more frequent HPV screening in people with immunosuppression, further investigation of the vaginal microbiome and access to sexual health services.
持续性感染致癌型人乳头瘤病毒(HPV)是宫颈癌发生的必要条件,但不是充分条件。行为、环境或合并症暴露可能促进或预防恶性转化。随机证据有限,描述这些关联的观察性研究的有效性仍不清楚。
在本次伞式综述中,我们检索了电子数据库,以确定评估风险或保护因素以及 HPV 感染、宫颈上皮内瘤变(CIN)、宫颈癌发病率和死亡率的观察性研究的荟萃分析。经过重新分析,根据一套预先设定的统计标准对证据进行分类和分级。使用 AMSTAR-2 评估质量。对于所有被评为弱证据或以上的关联,如果有可用的遗传工具,我们还进行了孟德尔随机化分析,以检查与宫颈癌风险相关的可改变暴露因素的潜在因果效应。本研究的方案已在 PROSPERO(CRD42020189995)上注册。
我们纳入了 50 项研究中 171 项不同暴露对比的荟萃分析。包括 HIV 感染在内的全身性免疫抑制(RR=2.20(95%CI=1.89-2.54))和炎症性肠病的免疫抑制药物(RR=1.33(95%CI=1.27-1.39)),以及阴道微生物组的改变(RR=1.59(95%CI=1.40-1.81)),这些证据都强烈且高度提示与 HPV 持续性感染、CIN 或宫颈癌相关。吸烟、性伴侣数量和初次妊娠年龄较小等因素也有高度提示性证据支持,并通过孟德尔随机化得到证实。
我们的主要分析支持全身性免疫抑制(HIV 感染、免疫抑制药物)和局部免疫抑制(阴道微生物组改变)与 HPV 和宫颈癌结局恶化风险增加之间的关联。孟德尔随机化证实了遗传预测的终生吸烟指数与宫颈癌之间的联系,以及初次妊娠年龄较小与宫颈癌之间的联系,同时也表明观察性证据可能隐藏了不同的固有偏见。这些证据加强了对免疫抑制人群进行更频繁 HPV 筛查、进一步研究阴道微生物组以及提供性健康服务的必要性。