Yoshimura Masataka, Yamaoka Hiroto, Ishikawa Mariko, Miwa Yusuke, Hayashi Toshihiko, Kaneoka Azumi, Murota Yasuhiro, Ito Kei, Kiyokawa Juri, Hirota Shin, Yamamoto Shinji
Department of Neurosurgery, Tsuchiura Kyodo General Hospital, Tsuchiura, Ibaraki, Japan.
Department of Endovascular Surgery, Tokyo Medical and Dental University, Tokyo, Japan.
J Neuroendovasc Ther. 2021;15(8):489-497. doi: 10.5797/jnet.oa.2021-0013. Epub 2021 May 13.
To examine the effectiveness of a newly developed emergency room (ER) protocol to treat patients with stroke and control the spread of SARS-CoV-2 by evaluating the door-to-picture time.
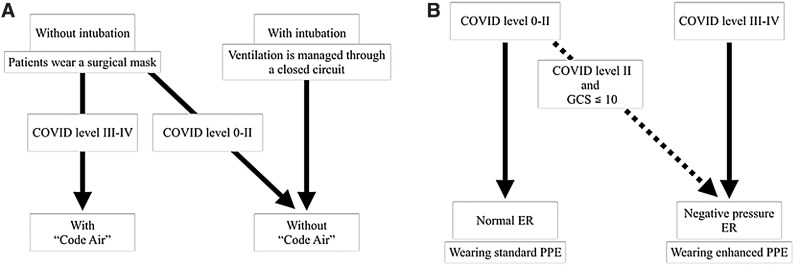
We retrospectively enrolled 126 patients who were transported to our ER by ambulance with suspected stroke between April 15 and October 31, 2020 (study group). A risk judgment system named the COVID level was introduced to classify the risk of infection as follows: level 0, no infection; I, infection unlikely; II, possible; III, probable; and IV, definite. Patients with COVID levels 0, I, or II and a Glasgow Coma Scale (GCS) score >10 were placed in a normal ER (nER) without atmospheric pressure control; the medical staff wore standard personal protective equipment (PPE) in such cases. Patients with COVID level II, III, or IV, and a GCS score of ≤10 were assigned to the negative pressure ER (NPER); the medical staff wore enhanced PPE for these cases. The validity of the protocol was assessed. The door-to-picture time of the study group was compared with that of 114 control patients who were transported with suspected stroke during the same period in 2019 (control group). The difference in the time for CT and MRI between the two groups was also compared. In the study group, the time spent in the nER and NPER was evaluated.
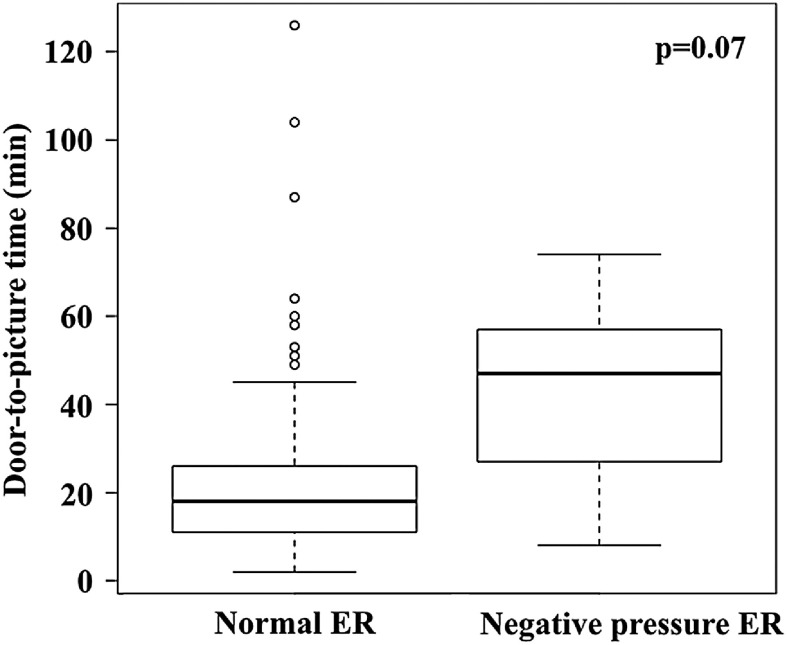
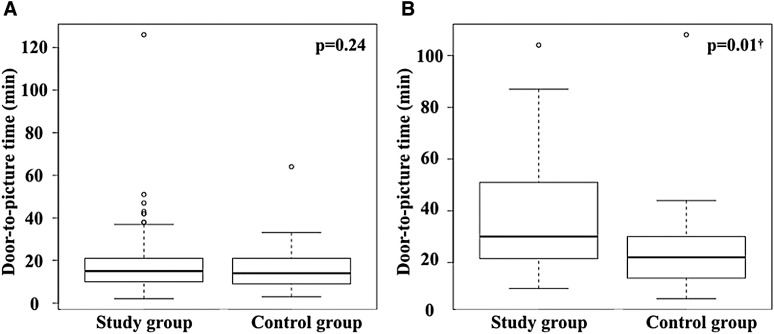
In all, 118 patients (93.7%) were classified as level I, 6 (4.8%) as level II, and 2 (1.6%) as level III. Only five patients (4.0%) were treated with NPER. Polymerase chain reaction tests were performed on 118 out of 126 patients (93.7%) and were negative. No significant differences were observed in age, sex, neurological severity, modalities of diagnostic imaging, and diagnosis compared with the control group. The median door-to-picture time was 18 (11-27.8) min in the study group and 15 (10-25) min in the control group (p = 0.08). No delay was found on CT (15 [10-21] vs. 14 [9-21] min, p = 0.24). In contrast, there was an 8-min delay for MRI (30 [21.8-50] vs. 22 [14-30] min, p = 0.01). The median door-to-picture time was 29 min longer in patients treated with NPER than in those treated with nER, although the difference was not significant due to the small number of patients (47 [27-57] vs. 18 [11-26] min, p = 0.07).
Our protocol could optimize the use of medical resources with only a 3-min delay in the door-to-picture time in an area without explosive outbreak. Unfortunately, the effectiveness of the protocol in preventing infection could not be verified because of the low incidence of COVID-19. When developing and modifying an institutional protocol, recognizing the outbreak status surrounding each institution is important.
通过评估从入院到完成影像检查的时间,研究一种新制定的急诊室(ER)方案治疗中风患者及控制SARS-CoV-2传播的有效性。
我们回顾性纳入了2020年4月15日至10月31日期间由救护车转运至我院急诊室、疑似中风的126例患者(研究组)。引入一种名为COVID等级的风险判断系统,将感染风险分类如下:0级,无感染;I级,不太可能感染;II级,可能感染;III级,很可能感染;IV级,确定感染。COVID等级为0级、I级或II级且格拉斯哥昏迷量表(GCS)评分>10分的患者被安置在无气压控制的普通急诊室(nER);此类情况下医护人员穿戴标准个人防护装备(PPE)。COVID等级为II级、III级或IV级且GCS评分≤10分的患者被分配至负压急诊室(NPER);此类情况下医护人员穿戴加强型PPE。评估该方案的有效性。将研究组从入院到完成影像检查的时间与2019年同期因疑似中风转运来的114例对照患者(对照组)进行比较。还比较了两组进行CT和MRI检查的时间差异。在研究组中,评估了在nER和NPER所花费的时间。
总共118例患者(93.7%)被分类为I级,6例(4.8%)为II级,2例(1.6%)为III级。仅5例患者(4.0%)在NPER接受治疗。126例患者中的118例(9