Samsky Marc D, Leverty Renee, Gray James M, Davis Alexandra, Fisher Brett, Govil Ashul, Stanis Tom, DeVore Adam D
Section of Cardiovascular Medicine, Yale University School of Medicine, New Haven, CT 06520, USA.
The Duke Clinical Research Institute, Durham, NC 27710, USA.
J Clin Med. 2023 Jul 14;12(14):4676. doi: 10.3390/jcm12144676.
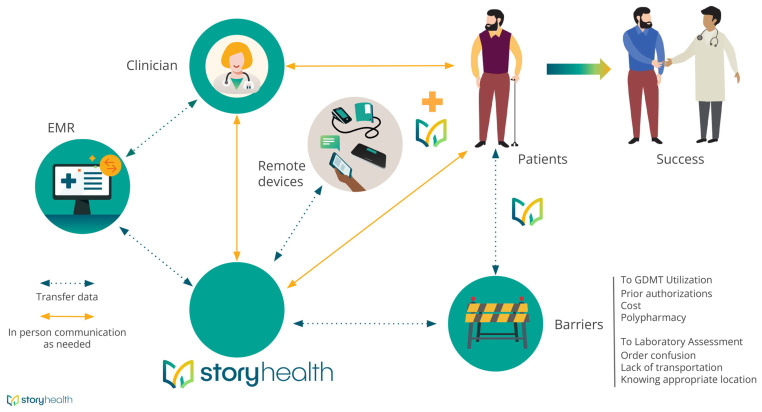
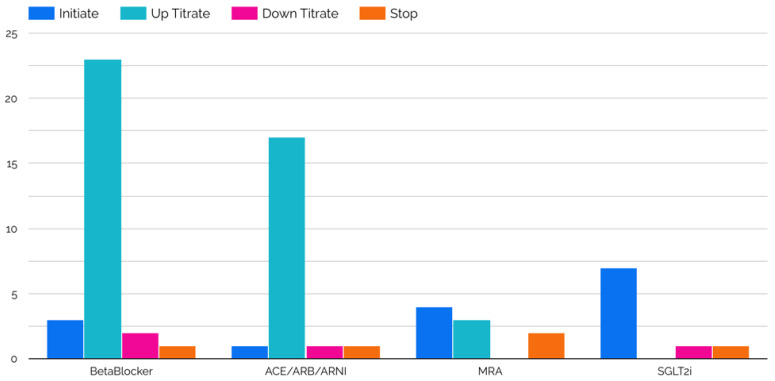
Use of guideline-directed medical therapy (GDMT) for treatment of heart failure with reduced ejection fraction (HFrEF) remains unacceptably low. The purpose of this study was to determine whether a digital health tool can augment GDMT for patients with HFrEF. Participants ≥ 18 years old with symptomatic HFrEF (left ventricular ejection fraction ≤ 40%) and with access to a mobile phone with internet were included. Participants were given a blood pressure cuff, instructed in its use, and given regular symptom surveys via cell-phone web-link. Data were transmitted to the Story Health web-based platform, and automated alerts were triggered based on pre-specified vital sign and laboratory data. Health coaches assisted patients with medication education, pharmacy access, and lab access through text messages and phone calls. GDMT titration plans were individually created in the digital platform by local clinicians based on entry vitals and labs. Twelve participants enrolled and completed the study. The median age and LVEF were 52.5 years (IQR, 46.5-63.5) and 25% (IQR, 22.5-35.5), respectively. There were 10 GDMT initiations, 52 up-titrations, and 13 down-titrations. Five participants engaged in focus-group interviews following study completion to understand first-hand perspectives regarding the use of digital tools to manage GDMT. Participants expressed comfort knowing that there were clinicians regularly reviewing their data. This alleviated concerns of uncertainty in daily living, led to an increased feeling of security, and empowered patients to understand decision-making regarding GDMT. Frequent medication changes, and the associated financial impact, were common concerns. Remote titration of GDMT for HFrEF is feasible and appears to be a patient-centered approach to care.
对于射血分数降低的心力衰竭(HFrEF)患者,使用指南指导的药物治疗(GDMT)的比例仍然低得令人无法接受。本研究的目的是确定一种数字健康工具是否可以增强HFrEF患者的GDMT。纳入年龄≥18岁、有症状的HFrEF(左心室射血分数≤40%)且能使用带互联网功能手机的参与者。为参与者提供了一个血压袖带,指导其使用方法,并通过手机网络链接定期进行症状调查。数据被传输到基于网络的Story Health平台,并根据预先设定的生命体征和实验室数据触发自动警报。健康教练通过短信和电话协助患者进行用药教育、获取药房服务和实验室检查。当地临床医生根据参与者的初始生命体征和实验室检查结果,在数字平台上为每个患者制定个性化的GDMT滴定计划。12名参与者登记并完成了研究。中位年龄和左心室射血分数分别为52.5岁(四分位间距,46.5 - 63.5)和25%(四分位间距,22.5 - 35.5)。共进行了10次GDMT起始治疗、52次剂量上调和13次剂量下调。5名参与者在研究完成后参加了焦点小组访谈,以了解他们对使用数字工具管理GDMT的第一手看法。参与者表示,知道有临床医生定期审查他们的数据让他们感到安心。这减轻了日常生活中的不确定性担忧,增强了安全感,并使患者能够理解有关GDMT的决策过程。频繁的药物调整及其相关的经济影响是常见的担忧。对HFrEF患者进行GDMT的远程滴定是可行的,并且似乎是一种以患者为中心的护理方法。