Balakumaran Kathir, Patil Aadhar, Marsh Shannon, Ingrassia Joseph, Kuo Chia-Ling, Jacoby Daniel Louis, Arora Sabeena, Soucier Richard
Department of Cardiology, University of Connecticut, Farmington, CT, United States of America.
Department of Internal Medicine, University of Connecticut, Farmington, CT, United States of America.
Int J Cardiol Heart Vasc. 2018 Nov 8;22:1-5. doi: 10.1016/j.ijcha.2018.10.003. eCollection 2019 Mar.
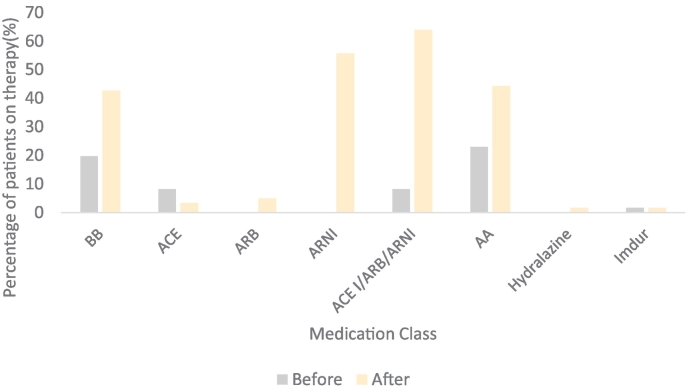
Heart failure is associated with recurrent hospitalizations and high mortality. Guideline directed medical treatment (GDMT), including beta blockers (BBs), angiotensin converting enzyme inhibitors (ACE-Is), angiotensin receptor blockers (ARBs) and aldosterone antagonists (AAs) has shown to improve outcomes. Current guidelines recommend the use of these medication classes at maximally tolerated dosages. Despite the evidence, < 25% of patients with heart failure with reduced left ventricular ejection fraction (HFrEF) are on the appropriate medical regimen titrated to the target doses. As such, we sought to assess the utility of a focused GDMT clinic to reduce this gap.
We conducted a retrospective chart review through existing patient data in a single center teaching hospital of patients referred to a focused GDMT clinic primarily staffed with heart failure trained nurse specialists, physician assistants and cardiologists. Management guidelines were developed with protocols for the initiation and uptitration of all therapeutic agents considered as GDMT.Our primary objective was to determine whether enrollment into a dedicated nursing led guideline directed medical therapy clinic would increase the proportion of patients with heart failure with reduced ejection fraction on appropriate medications as well as medication dosages in patients, the percentage of patients on the following medications and percentage at target doses: Renin-Angiotensin-Aldosterone System Blockers, Evidence Based Beta Blockers, and Aldosterone Antagonists. Our secondary objective was to determine if there was any clinical benefit on objective measures including renal function, hospital admissions, mortality and implantable defibrillator shocks.
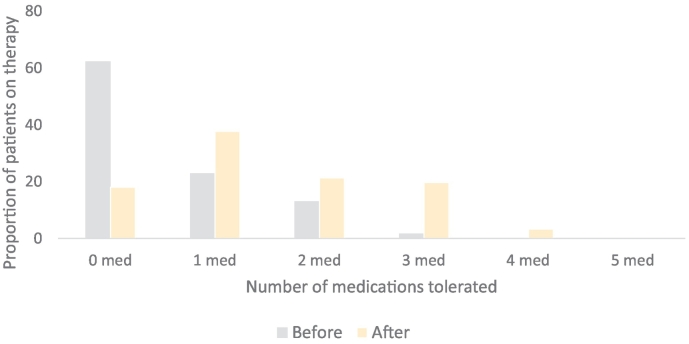
Between October 2015 and March 2017, 63 patients were identified by requisition forms, in which 61 were able to be identified based on legibility of identifying information. Mean duration of follow up was 264.44 ± 162.68 days over 7 ± 3.94 days. Mean ejection fraction was 21.8 ± 7.3%. New onset cardiomyopathies (diagnosed within 30 days) compiled 21% of the patient population while those with demonstrated cardiomyopathies (> 90 days) compiled 48% of the patient population. Patients with NYHA class III heart failure compiled 65% of the patient population.There was a statistically significant increase in the mean number of GDMT at any dose (2.31 ± 0.76 to 2.74 ± 0.66; p < 0.001) and mean number of GDMT at target doses (0.54 ± 0.79 to 1.52 ± 1.1; p < 0.001). Percentage of the population that were on no target doses at initial visit was 62% which was reduced to 18% after intervention.Clinical improvement was reflected in significant improvement in ejection fraction from 21.8 ± 7.8% to 36.2 ± 14.3% (p < 0.001). Increases in sodium and chloride were statistically small but significant. There a significant reduction in heart failure hospitalizations in comparison to a year prior to after the initial encounter in the clinic (p < 0.001).
This pilot study showed that a nurse directed GDMT titration program successfully increased the number of GDMT that patients were able to tolerate in a timely fashion, all the while enhancing ejection fraction, sodium and chloride levels, with a reduction in rehospitalization rates.
心力衰竭与反复住院和高死亡率相关。包括β受体阻滞剂(BBs)、血管紧张素转换酶抑制剂(ACE-Is)、血管紧张素受体阻滞剂(ARBs)和醛固酮拮抗剂(AAs)在内的指南指导药物治疗(GDMT)已显示可改善预后。当前指南推荐以最大耐受剂量使用这些药物类别。尽管有证据支持,但左心室射血分数降低的心力衰竭(HFrEF)患者中,只有不到25%的患者采用了滴定至目标剂量的适当药物治疗方案。因此,我们试图评估设立一个专注于GDMT的诊所来缩小这一差距的效用。
我们通过一家单中心教学医院的现有患者数据进行了回顾性病历审查,这些患者被转诊至一个专注于GDMT的诊所,该诊所主要由接受过心力衰竭培训的护士专家、医师助理和心脏病专家组成。制定了管理指南,其中包含所有被视为GDMT的治疗药物的起始和滴定方案。我们的主要目标是确定加入一个由护士主导的遵循指南的药物治疗诊所是否会增加射血分数降低的心力衰竭患者使用适当药物以及达到药物剂量目标的比例,包括使用以下药物的患者百分比和达到目标剂量的百分比:肾素 - 血管紧张素 - 醛固酮系统阻滞剂、循证β受体阻滞剂和醛固酮拮抗剂。我们的次要目标是确定在包括肾功能、住院、死亡率和植入式除颤器电击等客观指标上是否有任何临床益处。
在2015年10月至2017年3月期间,通过申请表确定了63例患者,其中61例根据识别信息的清晰度得以确认。平均随访时间为(264.44 ± 162.68)天,共(7 ± 3.94)次随访。平均射血分数为(21.8 ± 7.3)%。新发心肌病(在30天内诊断)占患者总数的21%,而确诊心肌病(> 90天)占患者总数的48%。纽约心脏协会(NYHA)III级心力衰竭患者占患者总数的65%。任何剂量的GDMT平均数量有统计学显著增加(从2.31 ± 0.76增加至2.74 ± 0.66;p < 0.001),目标剂量的GDMT平均数量也有统计学显著增加(从0.54 ± 0.79增加至1.52 ± 1.1;p < 0.001)。初诊时未达到目标剂量的患者比例为62%,干预后降至18%。临床改善表现为射血分数从(21.8 ± 7.8)%显著提高至(36.2 ± 14.3)%(p < 0.001)。钠和氯的增加在统计学上虽小但显著。与诊所初次就诊前一年相比,心力衰竭住院次数显著减少(p < 0.001)。
这项初步研究表明,由护士主导的GDMT滴定计划成功增加了患者能够及时耐受的GDMT数量,同时提高了射血分数、钠和氯水平,并降低了再住院率。