Amanzo-Vargas Maria Pia, Arellano-Veintemilla Tessy, González-Lagos Elsa, Echevarría Juan, Mejía Fernando, Graña Ana, Gotuzzo Eduardo
Facultad de Medicina, Universidad Peruana Cayetano Heredia, Lima 15102, Peru.
Instituto de Medicina Tropical "Alexander von Humboldt", Universidad Peruana Cayetano Heredia, Lima 15102, Peru.
Pathogens. 2023 Jun 24;12(7):869. doi: 10.3390/pathogens12070869.
In Peru, the estimated prevalence of human immunodeficiency virus (HIV) and human T-lymphotropic virus-1 (HTLV-1) co-infection has been reported to be as high as 18%. Despite the endemicity of HTLV-1 in Peru, few studies have assessed the impact of HIV/HTLV-1 co-infection. Our study compared socio-demographic and clinical characteristics, and mortality rates between HIV-infected and HIV/HTLV-1 co-infected patients.
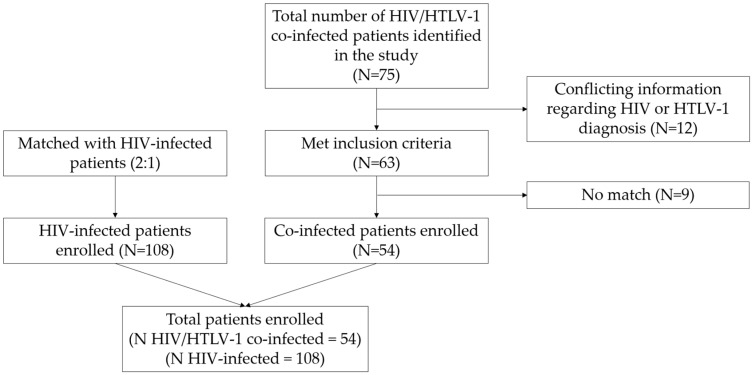
We reviewed the medical records of patients aged 18 years and older belonging to the HIV and HTLV-1 cohorts in Lima during a 30-year period: 1989-2019. Each HIV/HTLV-1 co-infected patient was randomly matched with two HIV-infected patients with similar characteristics (same sex, age ± 5 years, and same year of HIV diagnosis). Allegedly co-infected patients without a confirmatory diagnosis of HIV and HTLV-1 were excluded. Most of the patients in the HIV-infected group did not have a negative test result for HTLV-1 infection, so we used two probabilistic sensitivity analysis models to correct for potential HTLV-1 exposure misclassification bias in the group of HIV-infected patients.
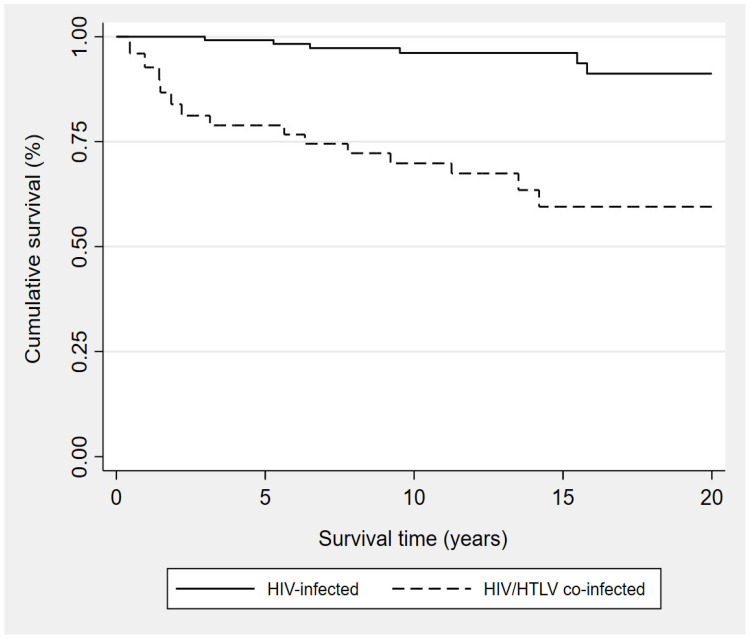
Of 162 patients enrolled, 54 were HIV/HTLV-1 co-infected and 108 were HIV-infected. The median age was 42 years (IQR = 34-51 years) and the majority were male (61.1%), single (44.4%), heterosexual (71%), born in Lima (58%), educated at the secondary school level (55.6%), and receiving antiretroviral treatment (91.4%). HIV/HTLV-1 co-infection was associated with an increased risk of death (HR: 11.8; 95% CI: 1.55-89.00; = 0.017) while antiretroviral treatment was associated with a decreased risk of death (HR: 0.03; 95% CI: 0.003-0.25; = 0.001). The overall mortality rate was 13.6 per 100 persons and the survival time for co-infected patients (median = 14.19 years) was significantly shorter than that of HIV-infected patients (median = 23.83 years) ( < 0.001).
HIV/HTLV-1 co-infected patients had a significantly shorter survival time compared to HIV-infected patients, suggesting that the immune alterations caused by HTLV-1 in CD4 cell count may have contributed to late initiation of antiretroviral treatment and prophylaxis against opportunistic infections over the decades, and thus reducing their benefits in these patients.
在秘鲁,据报道人类免疫缺陷病毒(HIV)与人类嗜T淋巴细胞病毒1型(HTLV-1)合并感染的估计患病率高达18%。尽管HTLV-1在秘鲁呈地方性流行,但很少有研究评估HIV/HTLV-1合并感染的影响。我们的研究比较了HIV感染患者与HIV/HTLV-1合并感染患者的社会人口学和临床特征以及死亡率。
我们回顾了1989年至2019年这30年间利马市HIV和HTLV-1队列中18岁及以上患者的病历。每例HIV/HTLV-1合并感染患者随机与两名具有相似特征(同性、年龄±5岁、HIV诊断年份相同)的HIV感染患者匹配。疑似合并感染但未确诊HIV和HTLV-1的患者被排除。HIV感染组的大多数患者没有HTLV-1感染的阴性检测结果,因此我们使用了两个概率敏感性分析模型来校正HIV感染患者组中潜在的HTLV-1暴露错误分类偏差。
在纳入的162例患者中,54例为HIV/HTLV-1合并感染,108例为HIV感染。中位年龄为42岁(四分位间距 = 34 - 51岁),大多数为男性(61.1%)、单身(44.4%)、异性恋(71%)、出生于利马(58%)、接受过中学教育(55.6%)且正在接受抗逆转录病毒治疗(91.4%)。HIV/HTLV-1合并感染与死亡风险增加相关(风险比:11.8;95%置信区间:1.55 - 89.00;P = 0.017),而抗逆转录病毒治疗与死亡风险降低相关(风险比:0.03;95%置信区间:0.003 - 0.25;P = 0.001)。总死亡率为每100人中有13.6例,合并感染患者的生存时间(中位值 = 14.19年)显著短于HIV感染患者(中位值 = 23.83年)(P < 0.001)。
与HIV感染患者相比,HIV/HTLV-1合并感染患者的生存时间显著缩短,这表明几十年来HTLV-1导致的CD4细胞计数免疫改变可能导致抗逆转录病毒治疗及机会性感染预防的延迟启动,从而降低了这些治疗对这些患者的益处。