Pickens Chiagozie I, Gao Catherine A, Bodner Justin, Walter James M, Kruser Jacqueline M, Donnelly Helen K, Donayre Alvaro, Clepp Katie, Borkowski Nicole, Wunderink Richard G, Singer Benjamin D
Division of Pulmonary and Critical Care Medicine, Department of Medicine, Feinberg School of Medicine, Northwestern University, Chicago, Illinois, USA.
Division of Allergy, Pulmonary and Critical Care Medicine, Department of Medicine, University of Wisconsin, Madison, Wisconsin, USA.
Open Forum Infect Dis. 2023 Jul 1;10(7):ofad336. doi: 10.1093/ofid/ofad336. eCollection 2023 Jul.
Clinical end points that constitute successful treatment in severe pneumonia are difficult to ascertain and vulnerable to bias. The utility of a protocolized adjudication procedure to determine meaningful end points in severe pneumonia has not been well described.
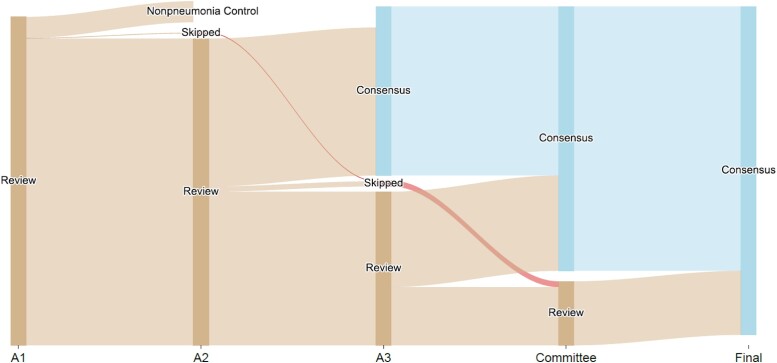
This was a single-center prospective cohort study of patients with severe pneumonia admitted to the medical intensive care unit. The objective was to develop an adjudication protocol for severe bacterial and/or viral pneumonia. Each episode of pneumonia was independently reviewed by 2 pulmonary and critical care physicians. If a discrepancy occurred between the 2 adjudicators, a third adjudicator reviewed the case. If a discrepancy remained after all 3 adjudications, consensus was achieved through committee review.
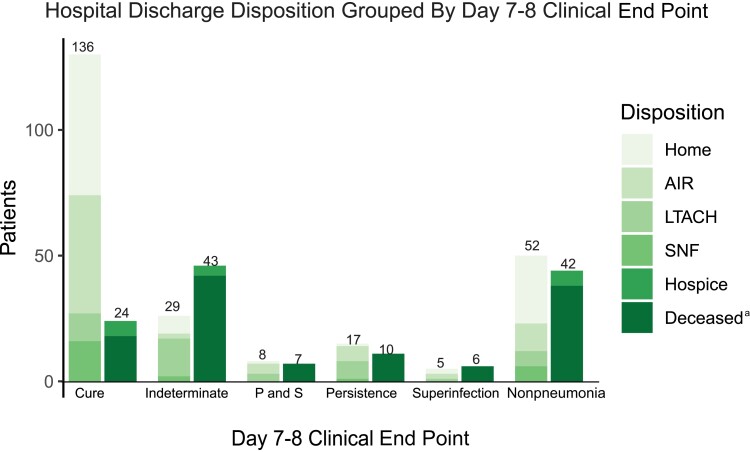
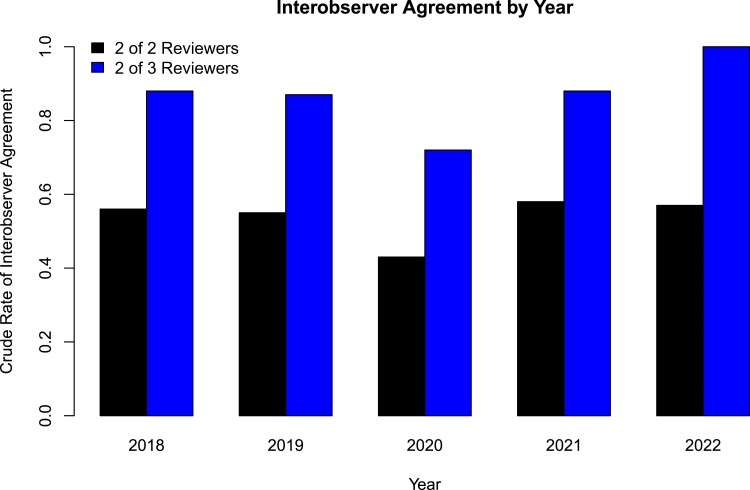
Evaluation of 784 pneumonia episodes during 593 hospitalizations achieved only 48.1% interobserver agreement between the first 2 adjudicators and 78.8% when agreement was defined as concordance between 2 of 3 adjudicators. Multiple episodes of pneumonia and presence of bacterial/viral coinfection in the initial pneumonia episode were associated with lower interobserver agreement. For an initial episode of bacterial pneumonia, patients with an adjudicated day 7-8 clinical impression of cure (compared with alternative impressions) were more likely to be discharged alive (odds ratio, 6.3; 95% CI, 3.5-11.6).
A comprehensive adjudication protocol to identify clinical end points in severe pneumonia resulted in only moderate interobserver agreement. An adjudicated end point of clinical cure by day 7-8 was associated with more favorable hospital discharge dispositions, suggesting that clinical cure by day 7-8 may be a valid end point to use in adjudication protocols.
构成重症肺炎成功治疗的临床终点难以确定且易受偏倚影响。尚未充分描述采用标准化裁决程序来确定重症肺炎中有意义的终点的效用。
这是一项针对入住医学重症监护病房的重症肺炎患者的单中心前瞻性队列研究。目的是制定一项针对重症细菌性和/或病毒性肺炎的裁决方案。每例肺炎均由2名肺科和重症医学医生独立评估。如果两名裁决者之间出现分歧,则由第三名裁决者复查该病例。如果在所有三次裁决后仍存在分歧,则通过委员会审查达成共识。
在593次住院期间对784例肺炎发作进行评估,前两名裁决者之间的观察者间一致性仅为48.1%,当将一致性定义为三名裁决者中有两名达成一致时,一致性为78.8%。多次肺炎发作以及初始肺炎发作时存在细菌/病毒混合感染与较低的观察者间一致性相关。对于初始细菌性肺炎发作,在第7 - 8天被判定临床治愈(与其他判定结果相比)的患者更有可能存活出院(比值比,6.3;95%置信区间,3.5 - 11.6)。
用于识别重症肺炎临床终点的综合裁决方案仅产生了中等程度的观察者间一致性。第7 - 8天判定临床治愈的终点与更有利的出院结局相关,这表明第7 - 8天临床治愈可能是裁决方案中一个有效的终点。