Division of Hepato-Biliary-Pancreatic, Minimally Invasive and Robotic Surgery and Kidney Transplantation, Department of Clinical Medicine and Surgery, Federico II University Hospital, via S. Pansini n. 5, Naples, Italy.
Nuffield Department of Surgical Sciences, University of Oxford, Oxford, UK.
Langenbecks Arch Surg. 2023 Jul 31;408(1):292. doi: 10.1007/s00423-023-03024-x.
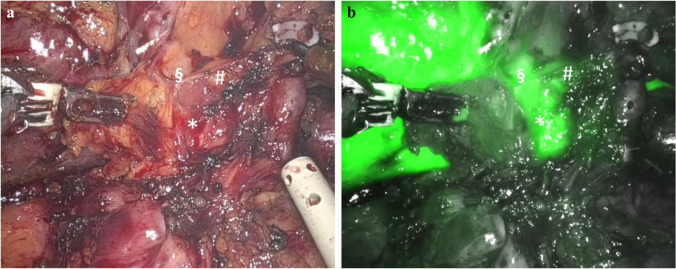
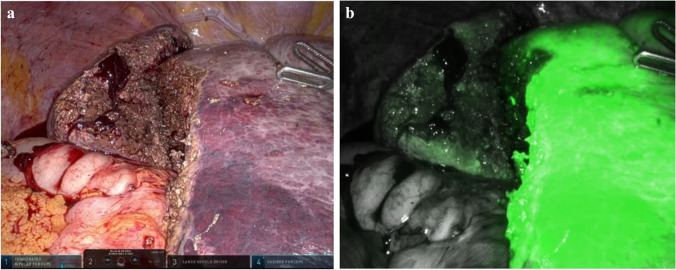
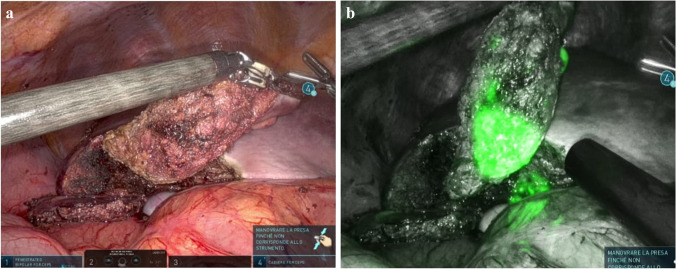
We aimed at exploring indocyanine green (ICG) fluorescence wide spectrum of applications in hepatobiliary surgery as can result particularly useful in robotic liver resections (RLR) in order to overcome some technical limitations, increasing safety, and efficacy.
We describe our experience of 76 RLR performed between March 2020 and December 2022 exploring all the possible applications of pre- and intraoperative ICG administration.
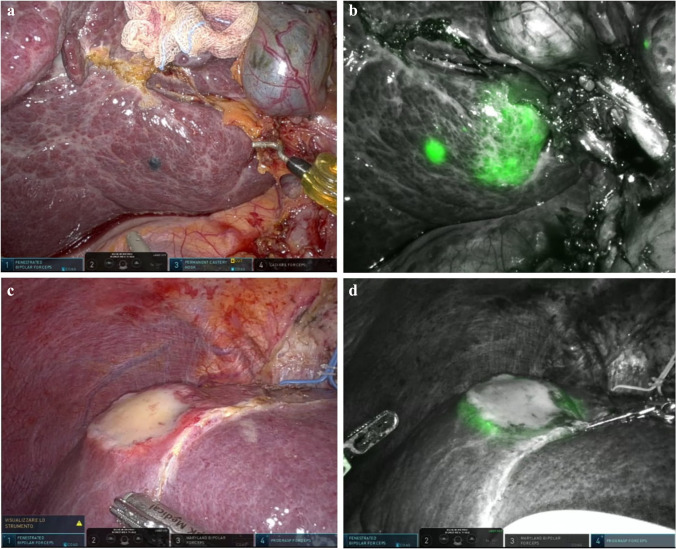
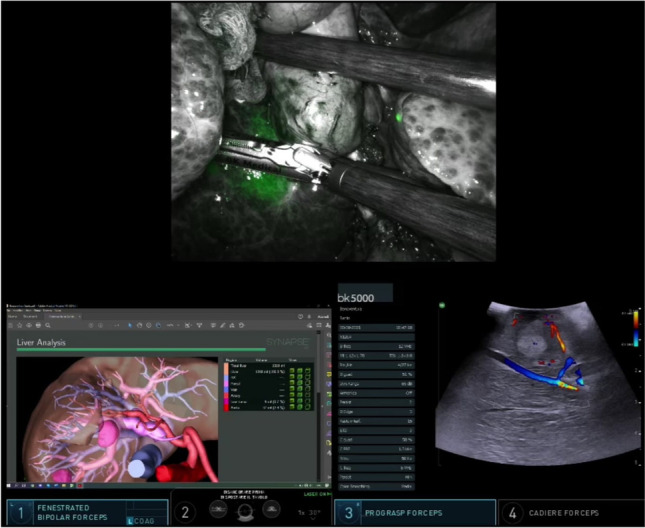
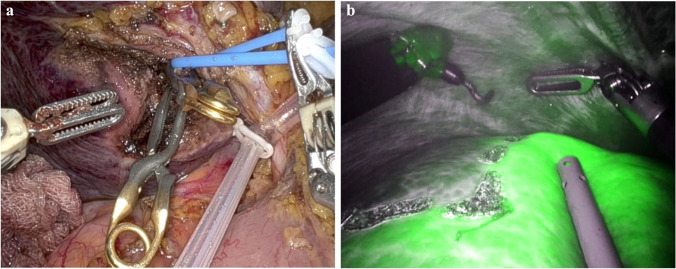
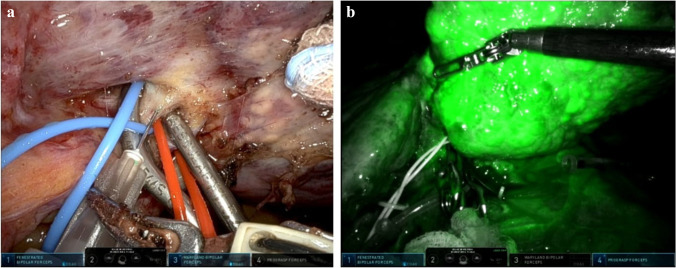
Hepatocellular carcinoma and colorectal liver metastases were the most common indications for RLR (34.2% and 26.7% of patients, respectively), and 51.3% of cases were complex resections with high IWATE difficulty scores. ICG was administered preoperatively in 61 patients (80.3%), intraoperatively in 42 patients (55.3%) and in both contexts in 25 patients (32.9%), with no observed adverse events. The most frequent ICG goal was to achieve tumor enhancement (59 patients, 77.6%), with a success rate of 94.9% and the detection of 3 additional malignant lesions. ICG facilitated evaluation of the resection margin for residual tumor and perfusion adequacy in 33.9% and 32.9% of cases, respectively, mandating a resection enlargement in 7.9% of patients. ICG fluorescence allowed the identification of the transection plane through negative staining in the 25% of cases. Vascular and biliary structures were visualized in 21.1% and 9.2% of patients, with a success rate of 81.3% and 85.7%, respectively.
RLR can benefit from the routine integration of ICG fluoresce evaluation according to each individual patient and condition-specific goals and issues, allowing liver functional assessment, anatomical and vascular evaluation, tumor detection, and resection margins assessment.
我们旨在探索吲哚菁绿(ICG)荧光在肝胆外科中的广泛应用,因为它在机器人肝切除(RLR)中可能特别有用,可以克服一些技术限制,提高安全性和疗效。
我们描述了我们在 2020 年 3 月至 2022 年 12 月期间进行的 76 例 RLR 的经验,探索了术前和术中 ICG 给药的所有可能应用。
肝细胞癌和结直肠癌肝转移是 RLR 最常见的适应证(分别为患者的 34.2%和 26.7%),51.3%的病例为高 IWATE 难度评分的复杂切除术。61 例患者(80.3%)术前给予 ICG,42 例(55.3%)术中给予 ICG,25 例(32.9%)同时给予 ICG,未观察到不良事件。最常见的 ICG 目标是实现肿瘤增强(59 例,77.6%),成功率为 94.9%,并检测到 3 个额外的恶性病变。ICG 有助于评估 33.9%和 32.9%的病例中残余肿瘤的切缘和灌注充足性,分别导致 7.9%的患者扩大切除。ICG 荧光在 25%的病例中通过负染识别出横断平面。21.1%和 9.2%的患者分别显示血管和胆道结构,成功率分别为 81.3%和 85.7%。
RLR 可以从常规整合 ICG 荧光评估中受益,根据每个患者和具体情况的目标和问题进行评估,允许进行肝功能评估、解剖和血管评估、肿瘤检测和切缘评估。