Department of Surgery, Leiden University Medical Center, Leiden, the Netherlands.
Department of Surgery, Amsterdam University Medical Center, University of Amsterdam, Amsterdam, the Netherlands.
JAMA Netw Open. 2024 Apr 1;7(4):e246548. doi: 10.1001/jamanetworkopen.2024.6548.
Unintended tumor-positive resection margins occur frequently during minimally invasive surgery for colorectal liver metastases and potentially negatively influence oncologic outcomes.
To assess whether indocyanine green (ICG)-fluorescence-guided surgery is associated with achieving a higher radical resection rate in minimally invasive colorectal liver metastasis surgery and to assess the accuracy of ICG fluorescence for predicting the resection margin status.
DESIGN, SETTING, AND PARTICIPANTS: The MIMIC (Minimally Invasive, Indocyanine-Guided Metastasectomy in Patients With Colorectal Liver Metastases) trial was designed as a prospective single-arm multicenter cohort study in 8 Dutch liver surgery centers. Patients were scheduled to undergo minimally invasive (laparoscopic or robot-assisted) resections of colorectal liver metastases between September 1, 2018, and June 30, 2021.
All patients received a single intravenous bolus of 10 mg of ICG 24 hours prior to surgery. During surgery, ICG-fluorescence imaging was used as an adjunct to ultrasonography and regular laparoscopy to guide and assess the resection margin in real time. The ICG-fluorescence imaging was performed during and after liver parenchymal transection to enable real-time assessment of the tumor margin. Absence of ICG fluorescence was favorable both during transection and in the tumor bed directly after resection.
The primary outcome measure was the radical (R0) resection rate, defined by the percentage of colorectal liver metastases resected with at least a 1 mm distance between the tumor and resection plane. Secondary outcomes were the accuracy of ICG fluorescence in detecting margin-positive (R1; <1 mm margin) resections and the change in surgical management.
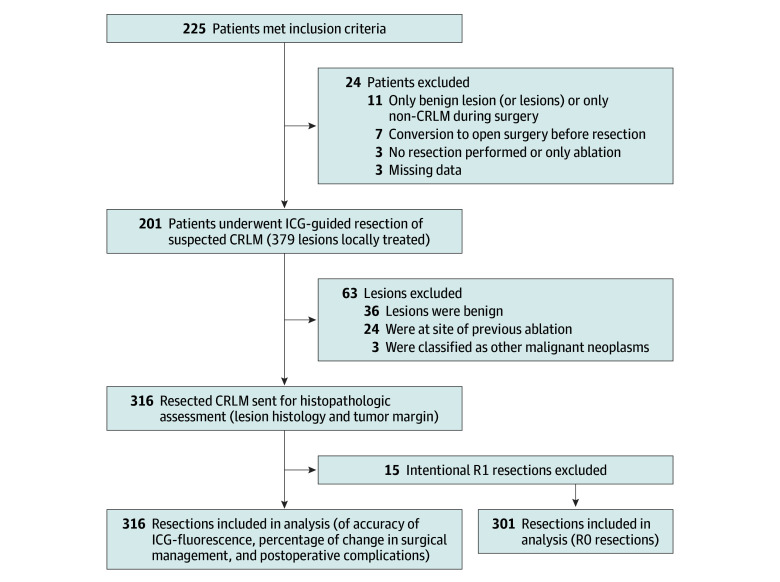
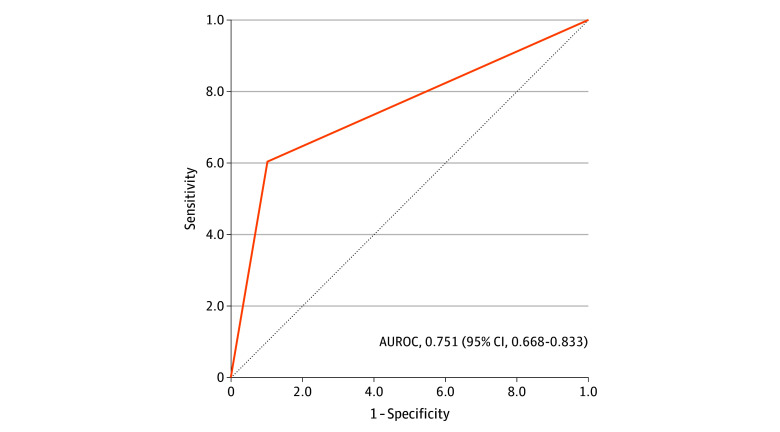
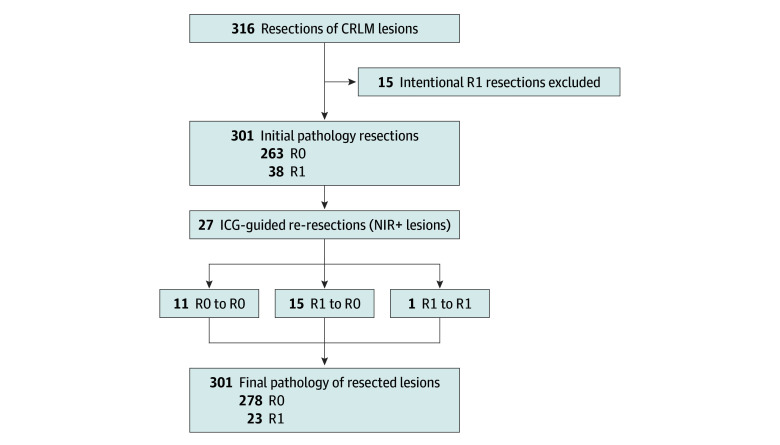
In total, 225 patients were enrolled, of whom 201 (116 [57.7%] male; median age, 65 [IQR, 57-72] years) with 316 histologically proven colorectal liver metastases were included in the final analysis. The overall R0 resection rate was 92.4%. Re-resection of ICG-fluorescent tissue in the resection cavity was associated with a 5.0% increase in the R0 percentage (from 87.4% to 92.4%; P < .001). The sensitivity and specificity for real-time resection margin assessment were 60% and 90%, respectively (area under the receiver operating characteristic curve, 0.751; 95% CI, 0.668-0.833), with a positive predictive value of 54% and a negative predictive value of 92%. After training and proctoring of the first procedures, participating centers that were new to the technique had a comparable false-positive rate for predicting R1 resections during the first 10 procedures (odds ratio, 1.36; 95% CI, 0.44-4.24). The ICG-fluorescence imaging was associated with changes in intraoperative surgical management in 56 (27.9%) of the patients.
In this multicenter prospective cohort study, ICG-fluorescence imaging was associated with an increased rate of tumor margin-negative resection and changes in surgical management in more than one-quarter of the patients. The absence of ICG fluorescence during liver parenchymal transection predicted an R0 resection with 92% accuracy. These results suggest that use of ICG fluorescence may provide real-time feedback of the tumor margin and a higher rate of complete oncologic resection.
在结直肠肝转移的微创外科手术中,肿瘤阳性切缘经常发生,这可能会对肿瘤学结果产生负面影响。
评估吲哚菁绿(ICG)荧光引导手术是否与微创结直肠肝转移手术中更高的根治性切除率相关,并评估 ICG 荧光预测切缘状态的准确性。
设计、设置和参与者:MIMIC(微创、ICG 指导结直肠癌肝转移患者的转移切除术)试验是在荷兰 8 个肝脏外科中心设计的前瞻性单臂多中心队列研究。计划于 2018 年 9 月 1 日至 2021 年 6 月 30 日期间对结直肠肝转移患者进行微创(腹腔镜或机器人辅助)切除术。
所有患者在手术前 24 小时内接受 10mgICG 的单次静脉推注。手术期间,ICG 荧光成像被用作超声和常规腹腔镜检查的辅助手段,以实时指导和评估切缘。ICG 荧光成像在肝实质横断期间和切除后直接在肿瘤床上进行,以实现肿瘤边缘的实时评估。横断过程中和切除后肿瘤床内无 ICG 荧光均为有利。
主要结局测量指标是根治(R0)切除率,定义为至少在肿瘤和切除平面之间有 1 毫米距离的结直肠肝转移的切除百分比。次要结局是 ICG 荧光检测边缘阳性(R1;<1mm 边缘)切除的准确性和手术管理的变化。
共纳入 225 例患者,其中 201 例(116 例[57.7%]为男性;中位年龄为 65 [IQR,57-72]岁),316 例经组织学证实的结直肠肝转移患者被纳入最终分析。总的 R0 切除率为 92.4%。在切除腔中对 ICG 荧光组织进行再次切除与 R0 百分比增加 5.0%相关(从 87.4%增加到 92.4%;P<0.001)。实时切缘评估的灵敏度和特异性分别为 60%和 90%(接受者操作特征曲线下面积,0.751;95%CI,0.668-0.833),阳性预测值为 54%,阴性预测值为 92%。在第一例手术的培训和监督之后,首次接受该技术的参与中心在预测 R1 切除方面具有相似的假阳性率(比值比,1.36;95%CI,0.44-4.24)。在 56 例(27.9%)患者中,ICG 荧光成像与术中手术管理的变化相关。
在这项多中心前瞻性队列研究中,ICG 荧光成像与肿瘤阴性切缘的切除率增加以及超过四分之一的患者手术管理的变化相关。肝实质横断过程中无 ICG 荧光可预测 R0 切除,准确率为 92%。这些结果表明,ICG 荧光的使用可能提供肿瘤边缘的实时反馈,并提高完整的肿瘤学切除率。