Department of Health Policy, London School of Economics and Political Science, London, UK
Center for Health Policy, University of the Witwatersrand, Johannesburg, South Africa.
BMJ Glob Health. 2023 Jul;8(7). doi: 10.1136/bmjgh-2023-012374.
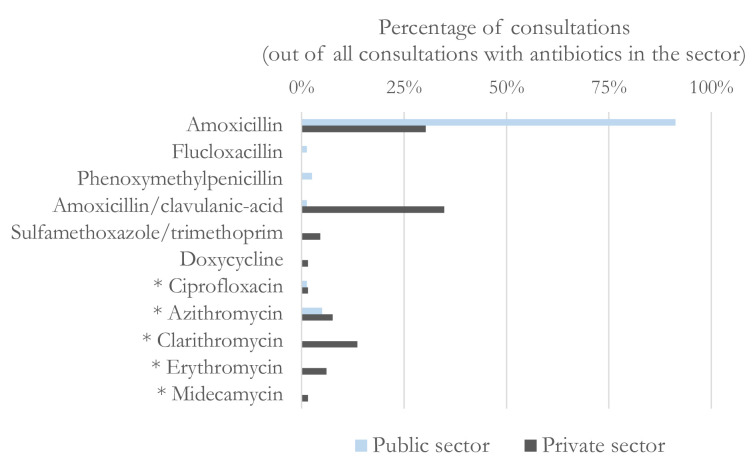
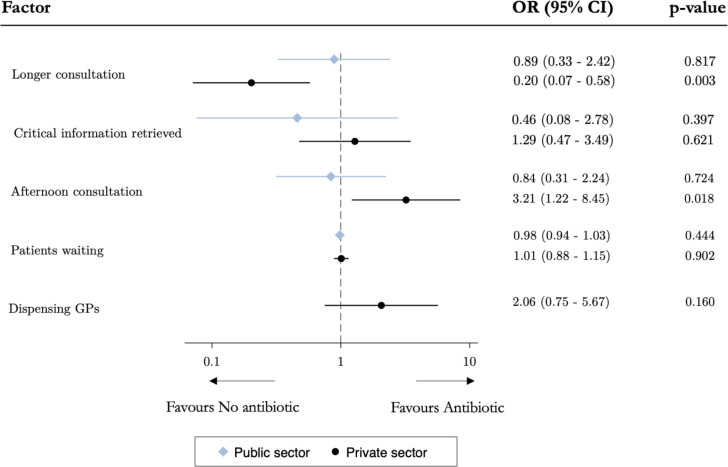
Although overprovision of antibiotics in primary care is a key driver of antibiotic resistance, little is known about its determinants in low-income and middle-income countries. Patient demand and financial incentives for providers are often held responsible for overprovision. Yet, inadequate provision exists in their absence and could be fuelled by quality of care issues and incorrect beliefs of providers regarding patients' expectations. We explored these issues in the private and public sector in South Africa, by conducting a cross-sectional study using standardised patients (SPs)-healthy individuals trained to portray a scripted clinical case to providers-presenting with symptoms of a viral respiratory infection in a sample of public and private sector clinics. We linked data from SP visits to rich survey data to compare the practices and their predictors in the two sectors. Unnecessary rates of antibiotics were similarly high in the public (78%) and private sector (67%), but private providers prescribed more antibiotics at higher risk of resistance development. In the private sector, overprescription of antibiotics diminished when consultations were more thorough, but increased for consultations scheduled later in the day, suggesting contrasting effects for provider effort and decision fatigue. We observed differences in beliefs that could be responsible for overprescription: in the public sector, a majority of providers (nurses) wrongly believed that antibiotics would help the patient recover more quickly. In the private sector, a majority of doctors thought patients would not come back if they did not receive antibiotics. Overall, this evidence suggests that different factors may be responsible for the high overprescribing rates of antibiotics in the public and private sectors. Tailored stewardship interventions are urgently needed that tackle providers' engrained habits and incorrect beliefs.
尽管初级保健中超量供应抗生素是抗生素耐药性的一个主要驱动因素,但对于低收入和中等收入国家的这种情况的决定因素知之甚少。患者的需求和提供者的经济激励通常被认为是造成过度供应的原因。然而,在这些因素不存在的情况下,供应不足仍然存在,并且可能是由于医疗质量问题以及提供者对患者期望的错误信念所助长的。我们通过在南非的公私部门进行横断面研究来探讨这些问题,该研究使用标准患者(SP)——经过培训可以向提供者描述编写好的临床病例的健康个体——在公共和私人诊所的样本中,为表现出病毒性呼吸道感染症状的患者提供服务。我们将 SP 就诊的数据与丰富的调查数据联系起来,以比较两个部门的实践及其预测因素。不必要的抗生素使用率在公共部门(78%)和私人部门(67%)同样很高,但私人提供者在更高的耐药风险下开了更多的抗生素。在私人部门,当咨询更加彻底时,抗生素的过度处方减少,但当天晚些时候安排的咨询增加,这表明提供者的努力和决策疲劳产生了相反的影响。我们观察到了可能导致过度处方的信念差异:在公共部门,大多数提供者(护士)错误地认为抗生素会帮助患者更快康复。在私人部门,大多数医生认为如果不给患者开抗生素,他们就不会再来就诊。总的来说,这一证据表明,公共部门和私人部门抗生素过度处方率高可能有不同的原因。迫切需要采取有针对性的管理干预措施,以解决提供者根深蒂固的习惯和错误信念。