Department of Anesthesiology, University of Arkansas for Medical Sciences, Little Rock.
Department of Anesthesiology, Duke University School of Medicine, Durham, North Carolina.
JAMA Netw Open. 2023 Aug 1;6(8):e2326710. doi: 10.1001/jamanetworkopen.2023.26710.
Dural-puncture epidural (DPE) and standard epidural are common modes of neuraxial labor analgesia. Little is known about conversion of DPE-initiated labor analgesia to surgical anesthesia for cesarean delivery.
To determine whether DPE provides a faster onset and better-quality block compared with the standard epidural technique for cesarean delivery.
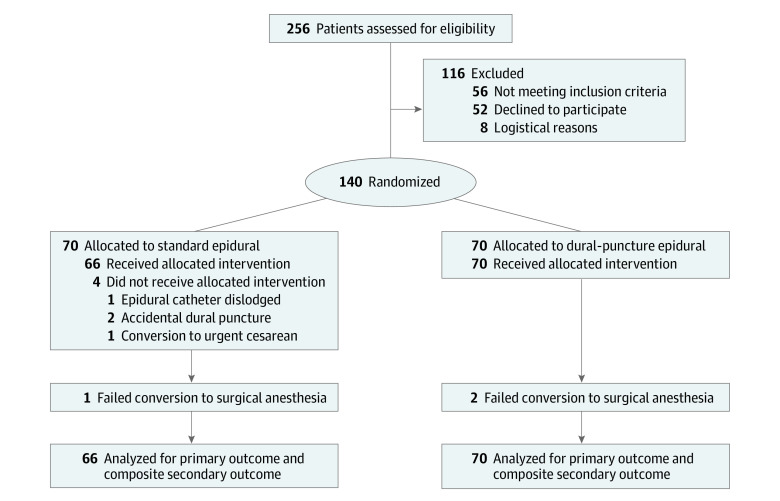
DESIGN, SETTING, AND PARTICIPANTS: This double-blind, randomized clinical trial was conducted between April 2019 and October 2022 at a tertiary care university hospital (University of Arkansas for Medical Sciences). Participants included women aged 18 years and older undergoing scheduled cesarean delivery with a singleton pregnancy.
Participants were randomized to receive DPE or standard epidural in the labor and delivery room. A T10 sensory block was achieved and maintained using a low concentration of bupivacaine with fentanyl through the epidural catheter until the time of surgery. Epidural extension anesthesia was initiated in the operating room.
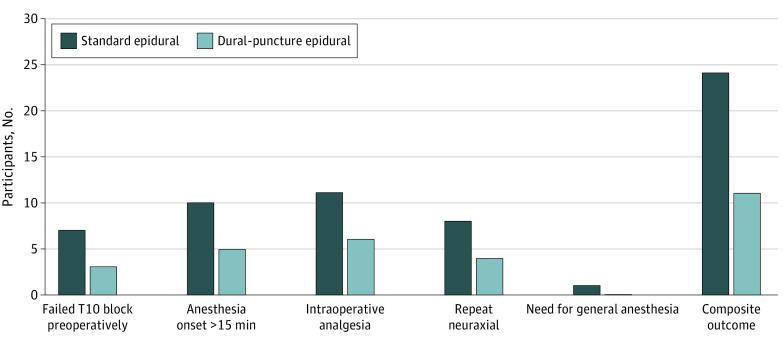
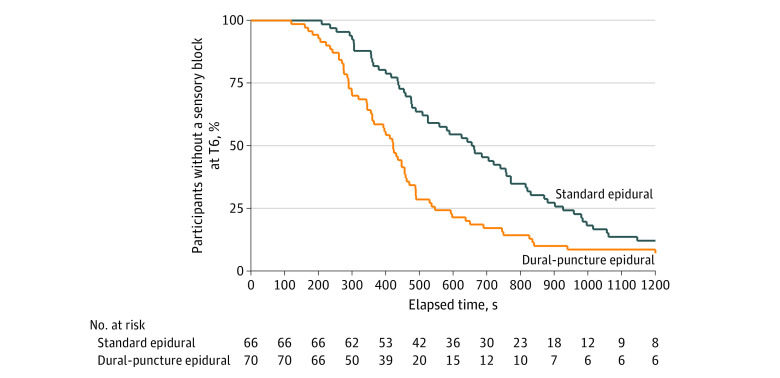
The primary outcome was the time taken from chloroprocaine administration to surgical anesthesia (T6 sensory block). The secondary outcome was the quality of epidural anesthesia, as defined by a composite of the following factors: (1) failure to achieve a T10 bilateral block preoperatively in the delivery room, (2) failure to achieve a surgical block at T6 within 15 minutes of chloroprocaine administration, (3) requirement for intraoperative analgesia, (4) repeat neuraxial procedure, and (5) conversion to general anesthesia.
Among 140 women (mean [SD] age, 30.1 [5.2] years), 70 were randomized to the DPE group, and 70 were randomized to the standard epidural group. The DPE group had a faster onset time to surgical anesthesia compared with the standard epidural group (median [IQR], 422 [290-546] seconds vs 655 [437-926] seconds; median [IQR] difference, 233 [104-369] seconds). The composite rates of lower quality anesthesia were 15.7% (11 of 70 women) in the DPE group and 36.3% (24 of 66 women) in the standard epidural group (odds ratio, 0.33; 95% CI, 0.14-0.74; P = .007).
Anesthesia initiated following a DPE technique resulted in faster onset and improved block quality during epidural extension compared with initiation with a standard epidural technique. Further studies are needed to confirm these findings in the setting of intrapartum cesarean delivery.
ClinicalTrials.gov Identifier: NCT03915574.
硬脊膜穿刺硬膜外(DPE)和标准硬膜外是常见的分娩镇痛方式。对于 DPE 诱导的分娩镇痛转为剖宫产手术麻醉,知之甚少。
确定 DPE 与标准硬膜外技术相比,在剖宫产时是否具有更快的起效时间和更好的阻滞质量。
设计、地点和参与者:这是一项 2019 年 4 月至 2022 年 10 月在三级保健大学医院(阿肯色大学医学科学分校)进行的双盲、随机临床试验。参与者包括年龄在 18 岁及以上、计划行剖宫产术的单胎妊娠女性。
参与者在产房被随机分配接受 DPE 或标准硬膜外麻醉。通过硬膜外导管给予低浓度布比卡因和芬太尼,以达到 T10 感觉阻滞,并维持至手术时。在手术室开始硬膜外延伸麻醉。
主要结局是从氯普鲁卡因给药到手术麻醉(T6 感觉阻滞)的时间。次要结局是硬膜外麻醉质量,定义为以下因素的综合:(1)在产房术前未达到 T10 双侧阻滞,(2)氯普鲁卡因给药后 15 分钟内未达到 T6 手术阻滞,(3)需要术中镇痛,(4)重复行神经轴突操作,(5)转为全身麻醉。
在 140 名女性(平均[标准差]年龄,30.1[5.2]岁)中,70 名被随机分配到 DPE 组,70 名被随机分配到标准硬膜外组。与标准硬膜外组相比,DPE 组的手术麻醉起效时间更快(中位数[IQR],422[290-546]秒与 655[437-926]秒;中位数[IQR]差异,233[104-369]秒)。DPE 组的麻醉质量较差的综合发生率为 15.7%(70 名女性中的 11 名),标准硬膜外组为 36.3%(66 名女性中的 24 名)(比值比,0.33;95%置信区间,0.14-0.74;P=0.007)。
与标准硬膜外技术相比,DPE 技术后开始的麻醉在硬膜外延伸期间起效更快,阻滞质量更高。需要进一步的研究来确认这些发现是否适用于产时剖宫产。
ClinicalTrials.gov 标识符:NCT03915574。