Massachusetts General Hospital, Department of Emergency Medicine, Boston, Massachusetts, USA.
Harvard Medical School, Boston, Massachusetts, USA.
West J Emerg Med. 2023 Jul 12;24(4):703-709. doi: 10.5811/westjem.59340.
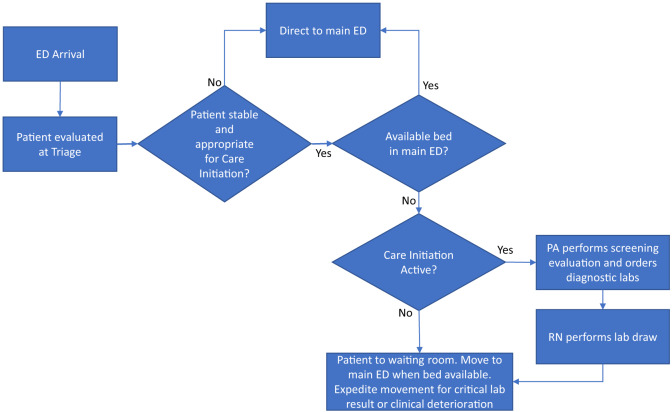
Emergency departments (ED) employ many strategies to address crowding and prolonged wait times. They include front-end Care Initiation and clinician-in-triage models that start the diagnostic and therapeutic process while the patient waits for a care space in the ED. The objective of this study was to quantify the impact of a Care Initiation model on resource utilization and operational metrics in the ED.
We performed a retrospective analysis of ED visits at our institution during October 2021. Baseline characteristics were compared with Chi-square and quantile regression. We used t-tests to calculate unadjusted difference in outcome measures, including number of laboratory tests ordered and average time patients spent in the waiting room and the ED treatment room, and the time from arrival until ED disposition. We performed propensity score analysis using matching and inverse probability weighting to quantify the direct impact of Care Initiation on outcome measures.
There were 2,407 ED patient encounters, 1,191 (49%) of whom arrived during the hours when Care Initiation was active. A total of 811 (68%) of these patients underwent Care Initiation, while the remainder proceeded directly to the main treatment area. Patients were more likely to undergo Care Initiation if they had lower acuity and lower risk of admission, and if the ED was busier as measured by the number of recent arrivals and percentage of occupied ED beds. After adjusting for patient-specific and department-level covariates, Care Initiation did not increase the number of diagnostic laboratory tests ordered. Care Initiation was associated with increased waiting room time by 1.8 hours and longer time from arrival until disposition by 1.3 hours, but with decreased time in the main treatment area by 0.6 hours, which represents a 15% reduction.
Care Initiation was associated with a 15% reduction in time spent in the main ED treatment area but longer waiting room time and longer time until ED disposition without significantly increasing the number of laboratory studies ordered. While previous studies produced similar results with Care Initiation models accessing all diagnostic modalities including imaging, our study demonstrates that a more limited Care Initiation model can still result in operational benefits for EDs.
急诊科(ED)采用多种策略来解决拥堵和延长等待时间的问题。其中包括前端护理启动和分诊医生模式,这些模式在患者等待 ED 治疗空间的同时开始诊断和治疗过程。本研究的目的是量化护理启动模式对 ED 资源利用和运营指标的影响。
我们对我院 2021 年 10 月期间的 ED 就诊进行了回顾性分析。使用卡方检验和分位数回归比较基线特征。我们使用 t 检验计算未调整的结果测量指标差异,包括实验室检查数量、患者在等候室和 ED 治疗室的平均时间,以及从到达至 ED 处置的时间。我们使用倾向评分分析进行匹配和逆概率加权,以量化护理启动对结果测量的直接影响。
共有 2407 例 ED 患者就诊,其中 1191 例(49%)在护理启动时段到达。共有 811 例(68%)患者接受了护理启动,其余患者直接进入主治疗区。如果患者的病情较轻、住院风险较低,并且 ED 较忙(根据最近到达的人数和占用的 ED 床位百分比衡量),那么他们更有可能接受护理启动。在调整患者特定和部门层面的协变量后,护理启动并没有增加诊断实验室检查的数量。护理启动与等候室时间增加 1.8 小时和从到达至处置的时间增加 1.3 小时有关,但与主治疗区时间减少 0.6 小时有关,减少了 15%。
护理启动与主 ED 治疗区时间减少 15%有关,但等候室时间延长,从到达至处置的时间延长,而实验室检查数量没有显著增加。虽然之前的研究表明护理启动模型可以访问所有诊断方式,包括影像学检查,会产生类似的结果,但我们的研究表明,更有限的护理启动模型仍然可以为 ED 带来运营效益。