Department of Cardiology, Zealand University Hospital, University of Copenhagen, Roskilde, Denmark.
Department of Cardiology, Herlev-Gentofte Hospital, University of Copenhagen, Hellerup, Denmark.
Diabetologia. 2023 Nov;66(11):2017-2029. doi: 10.1007/s00125-023-05977-6. Epub 2023 Aug 2.
AIMS/HYPOTHESIS: We aimed to examine whether individuals with initial omission of glucose-lowering drug treatment (GLDT), including those achieving initial remission of type 2 diabetes, may experience a higher risk of major adverse cardiovascular events (MACE) compared with well-controlled individuals on GLDT after a new type 2 diabetes diagnosis in real-world clinical practice. Furthermore, we examined whether a higher risk could be related to lower initiation of statins and renin-angiotensin system inhibitors (RASi).
In this cohort study, we used Danish registers to identify individuals with a first measured HbA between 48 and 57 mmol/mol (6.5-7.4%) from 2014 to 2020. Six months later, we divided participants into four groups according to GLDT and achieved HbA (<48 vs ≥48 mmol/mol [6.5%]): well-controlled and poorly controlled on GLDT; remission and persistent type 2 diabetes not on GLDT. We reported how much the standardised 5 year risk of MACE could be reduced for each group if initiation of statins and RASi was the same as in the well-controlled group on GLDT.
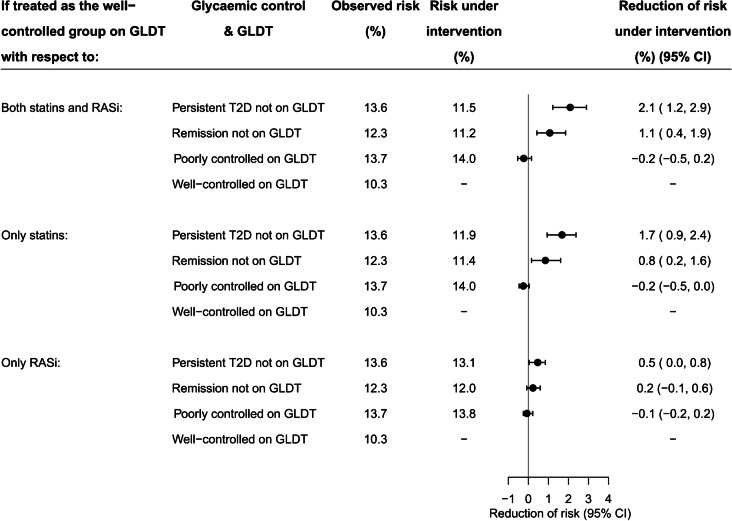
We included 14,221 individuals. Compared with well-controlled participants on GLDT, the 5 year standardised risk of MACE was higher in the three other exposure groups: by 3.3% (95% CI 1.6, 5.1) in the persistent type 2 diabetes group not on GLDT; 2.0% (95% CI 0.4, 3.7) in the remission group not on GLDT; and 3.5% (95% CI 1.3, 5.7) in the poorly controlled group on GLDT. Fewer individuals not on GLDT initiated statins and RASi compared with individuals on GLDT. If initiation of statins and RASi had been the same as in the well-controlled group on GLDT, participants not on GLDT could have reduced their risk of MACE by 2.1% (95% CI 1.2, 2.9) in the persistent type 2 diabetes group and by 1.1% (95% CI 0.4, 1.9) in the remission group.
CONCLUSIONS/INTERPRETATION: Compared with well-controlled individuals on GLDT, individuals not on initial GLDT had a higher 5 year risk of MACE, even among those achieving remission of type 2 diabetes. This may be related to lower use of statins and RASi.
目的/假设:我们旨在研究在现实临床实践中,对于新诊断的 2 型糖尿病患者,与持续接受降糖药物治疗(GLDT)且血糖控制良好的患者相比,初始未接受 GLDT 治疗(包括初始缓解的 2 型糖尿病患者)的患者,主要不良心血管事件(MACE)的风险是否更高。此外,我们还研究了这种更高的风险是否与他汀类药物和肾素-血管紧张素系统抑制剂(RASi)的起始使用率较低有关。
在这项队列研究中,我们使用丹麦登记处,从 2014 年至 2020 年,确定了首次测量的 HbA 在 48 至 57mmol/mol(6.5-7.4%)之间的个体。6 个月后,我们根据 GLDT 和 HbA 结果(<48 与≥48mmol/mol [6.5%])将参与者分为四组:持续接受 GLDT 治疗且血糖控制良好的组;持续接受 GLDT 治疗且血糖控制不佳的组;初始未接受 GLDT 治疗但 2 型糖尿病缓解的组;初始未接受 GLDT 治疗且 2 型糖尿病未缓解的组。我们报告了如果起始使用他汀类药物和 RASi 与持续接受 GLDT 且血糖控制良好的组相同,那么每个组的 MACE 5 年标准化风险可降低多少。
我们纳入了 14221 名个体。与持续接受 GLDT 治疗且血糖控制良好的参与者相比,其他三个暴露组的 MACE 5 年标准化风险更高:初始未接受 GLDT 治疗但 2 型糖尿病持续存在的组风险高 3.3%(95%CI,1.6-5.1);初始未接受 GLDT 治疗但 2 型糖尿病缓解的组风险高 2.0%(95%CI,0.4-3.7);持续接受 GLDT 治疗但血糖控制不佳的组风险高 3.5%(95%CI,1.3-5.7)。与持续接受 GLDT 治疗的个体相比,初始未接受 GLDT 治疗的个体起始他汀类药物和 RASi 的比例更低。如果起始使用他汀类药物和 RASi 与持续接受 GLDT 且血糖控制良好的组相同,那么初始未接受 GLDT 治疗的患者中,2 型糖尿病持续存在的组的 MACE 风险可降低 2.1%(95%CI,1.2-2.9),2 型糖尿病缓解的组的 MACE 风险可降低 1.1%(95%CI,0.4-1.9)。
结论/解释:与持续接受 GLDT 治疗且血糖控制良好的个体相比,即使在 2 型糖尿病缓解的患者中,初始未接受 GLDT 治疗的患者 5 年内发生 MACE 的风险也更高。这可能与他汀类药物和 RASi 的使用率较低有关。