Sánchez-Lozada Laura G, Madero Magdalena, Mazzali Marilda, Feig Daniel I, Nakagawa Takahiko, Lanaspa Miguel A, Kanbay Mehmet, Kuwabara Masanari, Rodriguez-Iturbe Bernardo, Johnson Richard J
Department of Cardio-Renal Physiopathology, Instituto Nacional de Cardiología "Ignacio Chavez", Mexico City, Mexico.
Division of Nephrology, Department of Medicine, Instituto Nacional de Cardiología "Ignacio Chavez", Mexico City, Mexico.
Clin Kidney J. 2023 Mar 23;16(8):1239-1248. doi: 10.1093/ckj/sfad058. eCollection 2023 Aug.
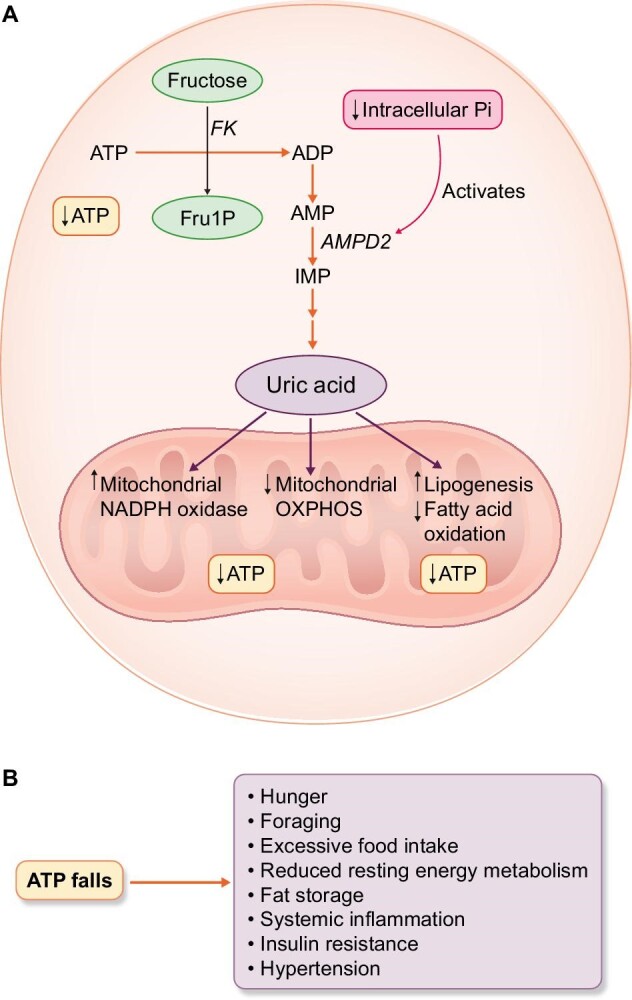
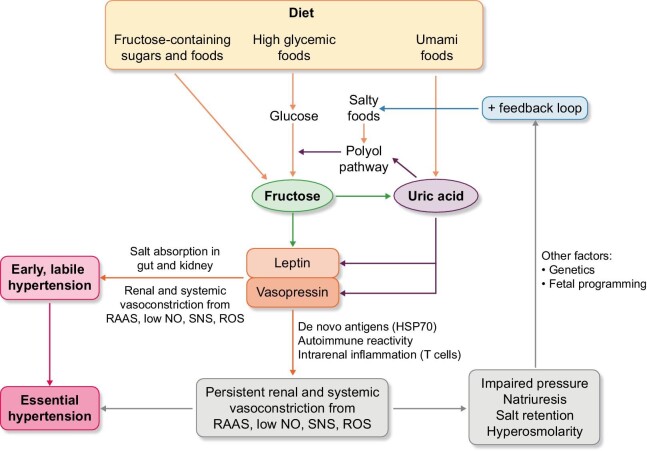
Despite its discovery more than 150 years ago, the cause of primary hypertension remains unknown. Most studies suggest that hypertension involves genetic, congenital or acquired risk factors that result in a relative inability of the kidney to excrete salt (sodium chloride) in the kidneys. Here we review recent studies that suggest there may be two phases, with an initial phase driven by renal vasoconstriction that causes low-grade ischemia to the kidney, followed by the infiltration of immune cells that leads to a local autoimmune reaction that maintains the renal vasoconstriction. Evidence suggests that multiple mechanisms could trigger the initial renal vasoconstriction, but one way may involve fructose that is provided in the diet (such as from table sugar or high fructose corn syrup) or produced endogenously. The fructose metabolism increases intracellular uric acid, which recruits NADPH oxidase to the mitochondria while inhibiting AMP-activated protein kinase. A drop in intracellular ATP level occurs, triggering a survival response. Leptin levels rise, triggering activation of the sympathetic central nervous system, while vasopressin levels rise, causing vasoconstriction in its own right and stimulating aldosterone production via the vasopressin 1b receptor. Low-grade renal injury and autoimmune-mediated inflammation occur. High-salt diets can amplify this process by raising osmolality and triggering more fructose production. Thus, primary hypertension may result from the overactivation of a survival response triggered by fructose metabolism. Restricting salt and sugar and hydrating with ample water may be helpful in the prevention of primary hypertension.
尽管原发性高血压在150多年前就已被发现,但其病因仍不明确。大多数研究表明,高血压涉及遗传、先天性或后天性风险因素,这些因素导致肾脏相对无法排泄肾脏中的盐分(氯化钠)。在此,我们回顾近期的研究,这些研究表明可能存在两个阶段,初始阶段由肾血管收缩驱动,导致肾脏出现轻度缺血,随后免疫细胞浸润,引发局部自身免疫反应,维持肾血管收缩。有证据表明,多种机制可能触发初始肾血管收缩,但一种方式可能涉及饮食中提供的果糖(如来自食糖或高果糖玉米糖浆)或内源性产生的果糖。果糖代谢会增加细胞内尿酸,尿酸会将NADPH氧化酶募集到线粒体,同时抑制AMP激活的蛋白激酶。细胞内ATP水平下降,触发生存反应。瘦素水平升高,触发交感中枢神经系统激活,而血管加压素水平升高,本身会导致血管收缩,并通过血管加压素1b受体刺激醛固酮生成。出现轻度肾损伤和自身免疫介导的炎症。高盐饮食可通过提高渗透压和触发更多果糖生成来放大这一过程。因此,原发性高血压可能源于果糖代谢触发的生存反应过度激活。限制盐和糖的摄入并大量饮水可能有助于预防原发性高血压。