Department of Renal Medicine, Northern Care Alliance NHS Foundation Trust, Salford, UK
Faculty of Biology Medicine and Health, The University of Manchester, Manchester, UK.
BMJ Open Qual. 2023 Aug;12(3). doi: 10.1136/bmjoq-2022-002188.
Chronic kidney disease (CKD) is estimated to affect more than 2.5 million adults in England, and this is expected to rise to 4.2 million by 2036 (1). Population-level digital healthcare systems have the potential to enable earlier detection of CKD providing an opportunity to introduce interventions that attenuate progression and reduce the risk of end-stage kidney disease (ESKD) and cardiovascular diseases (CVD). Services that can support patients with CKD, CVD, and diabetes mellitus (DM) have the potential to reduce fragmented clinical care and optimise pharmaceutical management.
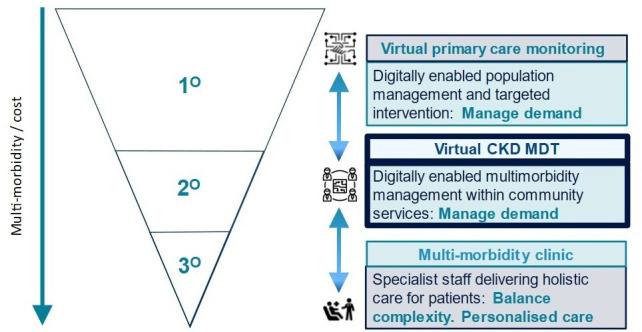
The Salford renal service has established an outpatient improvement programme which aims to address these issues via two projects. Firstly, the development of a CKD dashboard that can stratify patients by their kidney failure risk equation (KFRE) risk. High-risk patients would be invited to attend an outpatient clinic if appropriate. Specialist advice and guidance would be offered to primary care providers looking after patients with medium risk. Patients with lower risk would continue with standard care via their primary care provider unless there was another indication for a nephrology referral. The CKD dashboard identified 11546 patients (4.4% of the total adult population in Salford) with T2DM and CKD. The second project is the establishment of the Metabolic CardioRenal (MRC) clinic. It provided care for 209 patients in the first 8 months of its establishment with a total of 450 patient visits. Initial analysis showed clustering of cardiorenal metabolic diseases with 85% having CKD stages 3 and 4 and 73.2% having DM. In addition, patients had a significant burden of CVD with 50.2% having hypertension and 47.8% having heart failure.
There is a pressing need to create new outpatient models of care to tackle the rising epidemic of cardio-renal metabolic diseases. This model of service has potential benefits at both organisational and patient levels including improving patient management via risk stratification, increased care capacity and reduction of variation of care. Patients will benefit from earlier intervention, appropriate referral for care, reduction in CKD-related complications, and reduction in hospital visits and cardiovascular events. In addition, this combined digital and patient-facing model of care will allow rapid translation of advances in cardio-renal metabolic diseases into clinical practice.
据估计,慢性肾脏病(CKD)影响了英格兰超过 250 万成年人,到 2036 年这一数字预计将上升到 420 万(1)。人群水平的数字医疗保健系统有可能实现 CKD 的早期检测,从而有机会引入干预措施来减缓进展并降低终末期肾病(ESKD)和心血管疾病(CVD)的风险。能够为 CKD、CVD 和糖尿病(DM)患者提供支持的服务有可能减少临床护理的碎片化并优化药物管理。
索尔福德肾脏服务机构建立了一个门诊改进计划,该计划旨在通过两个项目来解决这些问题。首先,开发一个 CKD 仪表盘,可以根据他们的肾脏衰竭风险方程(KFRE)风险对患者进行分层。如果合适,高危患者将被邀请到门诊就诊。将向初级保健提供者提供照顾中危患者的专家建议和指导。低危患者将继续接受初级保健提供者的标准护理,除非有肾脏科转介的其他指征。CKD 仪表盘确定了 11546 名(索尔福德成年人口的 4.4%)患有 T2DM 和 CKD 的患者。第二个项目是建立代谢心肾(MRC)诊所。它在成立后的 8 个月内为 209 名患者提供了护理,共有 450 名患者就诊。初步分析显示,心肾代谢疾病存在聚集性,85%的患者患有 CKD 3 期和 4 期,73.2%的患者患有 DM。此外,患者的 CVD 负担很重,50.2%的患者患有高血压,47.8%的患者患有心力衰竭。
迫切需要创建新的门诊护理模式来应对日益流行的心肾代谢疾病。这种服务模式在组织和患者层面都具有潜在的好处,包括通过风险分层改善患者管理、增加护理能力以及减少护理的变异性。患者将受益于更早的干预、适当的护理转诊、减少 CKD 相关并发症以及减少就诊次数和心血管事件。此外,这种数字和面向患者的综合护理模式将允许将心肾代谢疾病方面的进展迅速转化为临床实践。