Bariatric Surgery Program, University Health Network, Toronto, Ontario, Canada.
Department of Psychiatry, University of Toronto, Toronto, Ontario, Canada.
JAMA Netw Open. 2023 Aug 1;6(8):e2327099. doi: 10.1001/jamanetworkopen.2023.27099.
Weight regain after bariatric surgery is associated with recurrence of obesity-related medical comorbidities and deterioration in quality of life. Developing efficacious psychosocial interventions that target risk factors, prevent weight regain, and improve mental health is imperative.
To determine the efficacy of a telephone-based cognitive behavioral therapy (tele-CBT) intervention at 1 year after bariatric surgery in improving weight loss, disordered eating, and psychological distress.
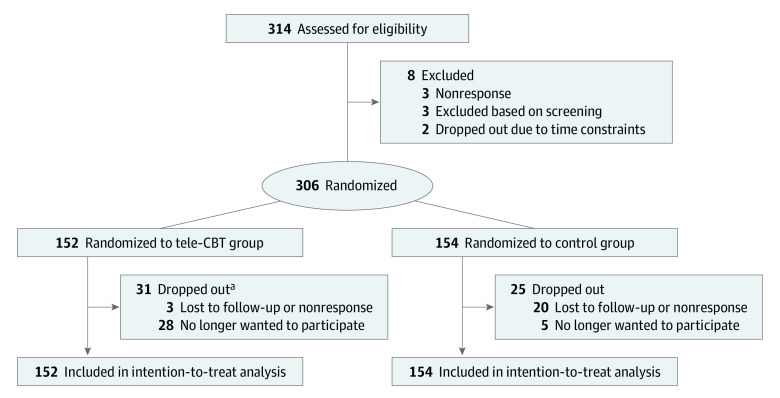
DESIGN, SETTING, AND PARTICIPANTS: This multisite randomized clinical trial was conducted at 3 hospital-based bariatric surgery programs, with recruitment between February 2018 and December 2021. Eligibility for participation was assessed among 314 adults at 1 year after bariatric surgery who were fluent in English and had access to a telephone and the internet. Patients with active suicidal ideation or poorly controlled severe psychiatric illness were excluded. Primary and secondary outcome measures were assessed at baseline (1 year after surgery), after the intervention (approximately 15 months after surgery), and at 3-month follow-up (approximately 18 months after surgery). Data were analyzed from January to February 2023.
The tele-CBT intervention consisted of 6 weekly 1-hour sessions and a seventh booster session 1 month later. The control group received standard postoperative bariatric care.
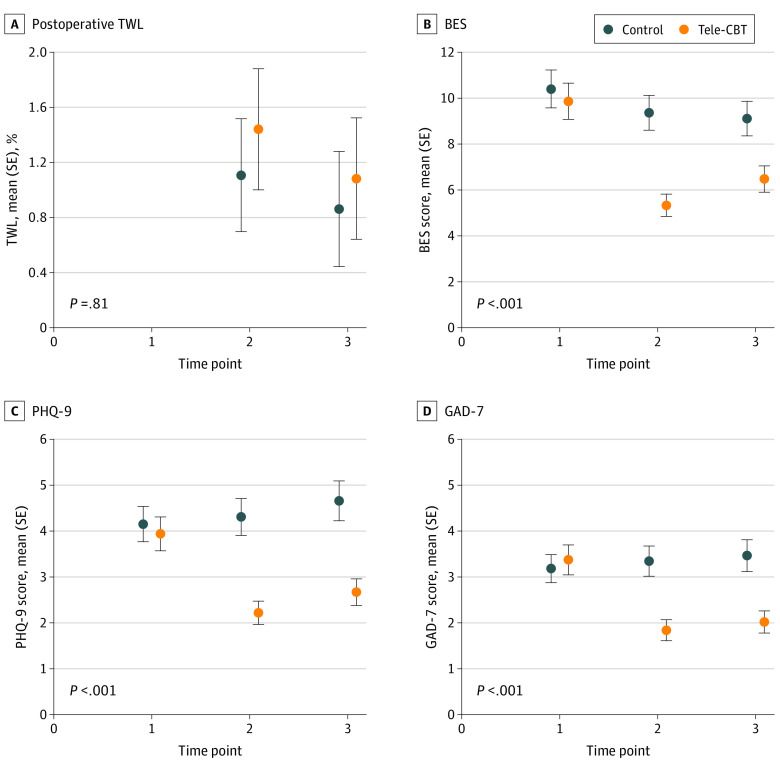
The primary outcome was postoperative percentage total weight loss. Secondary outcomes were disordered eating (Binge Eating Scale [BES] and Emotional Eating Scale [EES]) and psychological distress (Patient Health Questionnaire-9 item scale [PHQ-9] and Generalized Anxiety Disorder-7 item scale [GAD-7]). The hypotheses and data-analytic plan were developed prior to data collection.
Among 306 patients 1 year after bariatric surgery (255 females [83.3%]; mean [SD] age, 47.55 [9.98] years), there were 152 patients in the tele-CBT group and 154 patients in the control group. The group by time interaction for percentage total weight loss was not significant (F1,160.61 = 2.09; P = .15). However, there were significant interactions for mean BES (F2,527.32 = 18.73; P < .001), EES total (F2,530.67 = 10.83; P < .001), PHQ-9 (F2,529.93 = 17.74; P < .001), and GAD-7 (F2,535.16 = 15.29; P < .001) scores between the tele-CBT group and control group across all times.
This study found that tele-CBT delivered at 1 year after surgery resulted in no change in short-term weight outcomes but improved disordered eating and psychological distress. The impact of these psychosocial improvements on longer-term weight outcomes is currently being examined as part of this longitudinal multisite randomized clinical trial.
ClinicalTrials.gov Identifier: NCT03315247.
减重手术后体重反弹与肥胖相关的医疗合并症的复发和生活质量的恶化有关。开发针对风险因素、预防体重反弹和改善心理健康的有效心理社会干预措施是当务之急。
确定在减重手术后 1 年通过电话进行认知行为疗法(电话-CBT)干预对改善体重减轻、饮食失调和心理困扰的效果。
设计、地点和参与者:这项多中心随机临床试验在 3 家医院的减重手术项目中进行,招募时间为 2018 年 2 月至 2021 年 12 月。术后 1 年对 314 名接受英语流利并可使用电话和互联网的成年人进行了参与评估。排除有自杀意念或严重精神病控制不佳的患者。主要和次要结局评估在基线(手术 1 年后)、干预后(手术约 15 个月后)和 3 个月随访(手术约 18 个月后)进行。数据分析于 2023 年 1 月至 2 月进行。
电话-CBT 干预包括 6 次每周 1 小时的会议和 1 个月后的第 7 次强化会议。对照组接受标准的术后减重护理。
主要结局是术后体重总减轻百分比。次要结局是饮食失调(暴食症量表[BES]和情绪进食量表[EES])和心理困扰(患者健康问卷-9 项量表[PHQ-9]和广泛性焦虑障碍-7 项量表[GAD-7])。假设和数据分析计划是在数据收集之前制定的。
在 306 名术后 1 年的减重手术患者(255 名女性[83.3%];平均[SD]年龄,47.55[9.98]岁)中,电话-CBT 组有 152 名患者,对照组有 154 名患者。体重总减轻百分比的组间时间交互作用不显著(F1,160.61=2.09;P=0.15)。然而,BES 平均评分(F2,527.32=18.73;P<0.001)、EES 总分(F2,530.67=10.83;P<0.001)、PHQ-9 评分(F2,529.93=17.74;P<0.001)和 GAD-7 评分(F2,535.16=15.29;P<0.001)在电话-CBT 组和对照组之间的所有时间点均存在显著交互作用。
这项研究发现,在手术后 1 年进行电话-CBT 干预并未导致短期体重结果的变化,但改善了饮食失调和心理困扰。这些心理社会改善对长期体重结果的影响目前正在作为这项纵向多中心随机临床试验的一部分进行检查。
ClinicalTrials.gov 标识符:NCT03315247。