Solberg Ole Geir, Aaberge Lars, Bosse Gerhard, Ueland Thor, Gullestad Lars, Aukrust Pål, Stavem Knut
Department of Cardiology, Oslo University Hospital, Oslo, Norway.
Department of Radiology, Oslo University Hospital, Oslo, Norway.
ESC Heart Fail. 2023 Oct;10(5):3216-3222. doi: 10.1002/ehf2.14461. Epub 2023 Aug 3.
The aim of this study was to determine microvascular function in the acute phase of Takotsubo syndrome (TTS) and to identify inflammatory mediators that could reflect TTS-induced pathology.
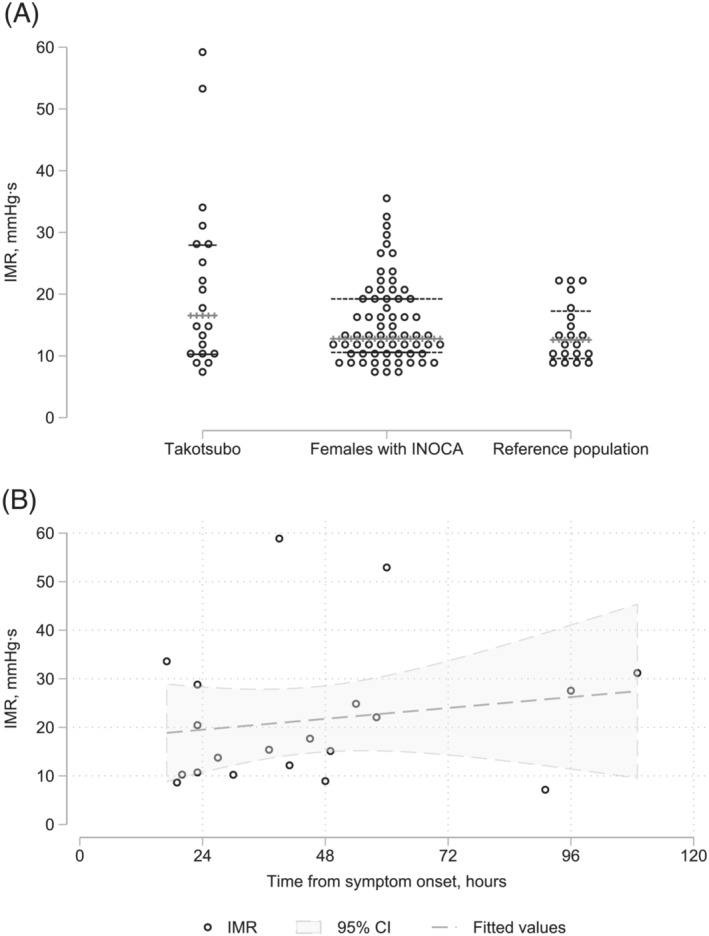
The study included 20 females [median age 65 years; interquarile range (IQR) = 58-70 years] with TTS according to the Mayo diagnostic criteria. During heart catheterization, we determined the index of microvascular resistance (IMR) and drew blood samples almost simultaneously from the aorta and coronary sinus. Cardiac magnetic resonance imaging (MRI) was done in the acute phase. We present descriptive coronary physiology and cardiac MRI data and compare inflammatory biomarkers between samples from the aorta, coronary sinus, and venous samples after 3 months using the Wilcoxon signed-rank test. For comparison, we also analysed the actual biomarkers in venous blood from 15 healthy female controls. A supplementary analysis explored Spearman's rank correlation between the inflammatory biomarkers, IMR, MRI data, and cardiac biomarkers. The median IMR was 16.5 mmHg·s (IQR = 10.5-28.2 mmHg·s), which was only slightly higher than that in the reference populations. Seven (35%) of the study subjects had IMR > 25 mmHg·s, suggesting a microvascular dysfunction. IMR was not affected by time from symptom onset. According to MRI, the apical region of the left ventricle was affected in 65% of the subjects. The median ejection fraction was 41% (IQR = 31-48%). Biomarker analyses revealed elevation of markers for extracellular matrix remodelling and fibrosis, inflammation, immune activation, and upstream inflammation as compared with healthy controls. Only the levels of interleukin (IL)-1 receptor antagonist and soluble T-cell immunoglobulin mucin domain-3 (sTIM-3) were higher in the coronary sinus than in the aorta. No variable was significantly correlated with IMR. The IL-6 level in the aorta was inversely correlated with the left ventricular ejection fraction. Growth differentiation factor-15, osteoprotegerin, and von Willebrand factor levels in both aorta and coronary sinus were positively correlated with N-terminal-pro-brain-natriuretic peptide, while the correlations of IL-6 and sTIM-3 with N-terminal-pro-brain-natriuretic peptide were restricted to the aorta and coronary sinus, respectively. While most of the markers were within normal limits after 3 months, matrix metalloproteinase-9 increased during follow-up to reach levels higher than those in the healthy controls.
The median IMR was only slightly elevated in this study, but about one-third of the patients had values indicating microvascular dysfunction. The present study supports the involvement of several inflammatory pathways in TTS, including monocyte/macrophage activation, with sTIM-3 as a potential novel marker.
本研究旨在确定应激性心肌病(TTS)急性期的微血管功能,并识别可反映TTS所致病理变化的炎症介质。
本研究纳入了20名符合梅奥诊断标准的女性患者[年龄中位数65岁;四分位间距(IQR)=58 - 70岁]。在心脏导管插入术期间,我们测定了微血管阻力指数(IMR),并几乎同时从主动脉和冠状窦采集血样。在急性期进行了心脏磁共振成像(MRI)检查。我们呈现了描述性的冠状动脉生理学和心脏MRI数据,并使用Wilcoxon符号秩检验比较了主动脉、冠状窦样本以及3个月后静脉样本之间的炎症生物标志物。为作比较,我们还分析了15名健康女性对照者静脉血中的实际生物标志物。一项补充分析探讨了炎症生物标志物、IMR、MRI数据和心脏生物标志物之间的Spearman等级相关性。IMR中位数为16.5 mmHg·s(IQR = 10.5 - 28.2 mmHg·s),仅略高于参考人群。7名(35%)研究对象的IMR > 25 mmHg·s,提示微血管功能障碍。IMR不受症状发作时间的影响。根据MRI检查,65%的研究对象左心室心尖区域受到影响。射血分数中位数为41%(IQR = 31 - 48%)。生物标志物分析显示,与健康对照者相比,细胞外基质重塑和纤维化、炎症、免疫激活以及上游炎症的标志物水平升高。仅白细胞介素(IL)-1受体拮抗剂和可溶性T细胞免疫球蛋白粘蛋白结构域-3(sTIM-3)在冠状窦中的水平高于主动脉。没有变量与IMR显著相关。主动脉中的IL-6水平与左心室射血分数呈负相关。主动脉和冠状窦中的生长分化因子-15、骨保护素和血管性血友病因子水平均与N末端脑钠肽前体呈正相关,而IL-6和sTIM-3与N末端脑钠肽前体的相关性分别仅限于主动脉和冠状窦。虽然大多数标志物在3个月后处于正常范围内,但基质金属蛋白酶-9在随访期间升高,达到高于健康对照者的水平。
本研究中IMR中位数仅略有升高,但约三分之一的患者其值表明存在微血管功能障碍。本研究支持多种炎症途径参与TTS,包括单核细胞/巨噬细胞激活,sTIM-3作为一种潜在的新型标志物。