School of Business and Economics, Talma Institute / VU University Amsterdam, Section Health Economics, De Boelelaan 1085, 1081 HV, Amsterdam, The Netherlands.
Dutch Healthcare Authority (NZa), Newtonlaan 1-41, 3584, BX, Utrecht, The Netherlands.
Eur J Health Econ. 2024 Jul;25(5):731-741. doi: 10.1007/s10198-023-01615-5. Epub 2023 Aug 9.
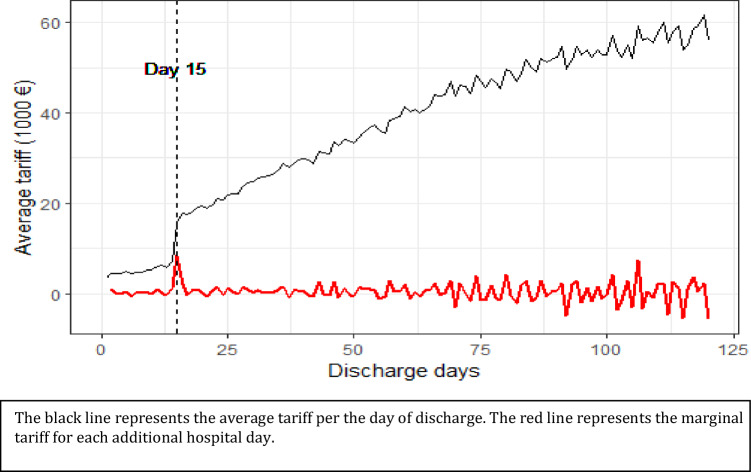
Non-linear reimbursement contracts in healthcare have been increasingly used to quantify providers' responses to financial incentives. In the present research, we utilize a large one-off increase in the reimbursement of rehabilitation care to assess to what extent providers are willing to modify their treating behavior to maximize profits. In order to disincentivize the use of short inpatient stays for rehabilitation care, Dutch policy-makers have instated a two-part stepwise tariff-schedule. A lower tariff-schedule is applied for short hospital stays (≤ 14 days), while a higher tariff-schedule is utilized for longer treatments. Switching from one schedule to the other at day 15 of inpatient care leads to a sudden and large increase in tariffs. We show that, for most care-types, patients are seldom treated in an inpatient setting for less than 15 days, while the majority of patients are discharged after the threshold. Therefore, we conclude that the financial incentive at day 15 leads to considerable distortions in treatment. However, instead of discharging all patients at the threshold point where marginal tariffs are maximized, providers tend to continue treatment indicating altruistic behavior. As healthcare payment systems move away from piecewise reimbursement (e.g., fee-for-service arrangements), and services are increasingly 'lumped' together into e.g., DRGs and bundled payments, the likelihood of such discontinuities in tariff-schedules radically increases. Our research illustrates how such discontinuities in reimbursements can lead to distortions in the amount of healthcare provided contributing to the debate on optimal healthcare contracting design.
医疗保健中的非线性报销合同越来越多地被用于量化提供者对财务激励的反应。在本研究中,我们利用康复护理报销的一次性大幅增加来评估提供者在多大程度上愿意改变他们的治疗行为以实现利润最大化。为了抑制康复护理的短期住院使用,荷兰政策制定者实施了两部分逐步递增的费率表。对于短期住院(≤14 天),采用较低的费率表,而对于较长的治疗则采用较高的费率表。在住院治疗的第 15 天从一个计划切换到另一个计划会导致关税的突然大幅增加。我们表明,对于大多数护理类型,患者很少在住院环境中接受少于 15 天的治疗,而大多数患者在阈值后出院。因此,我们得出结论,第 15 天的财务激励导致治疗出现相当大的扭曲。然而,提供者并没有在边际关税最大化的阈值点将所有患者出院,而是倾向于继续治疗,表明存在利他行为。随着医疗保健支付系统从分段报销(例如,按服务付费安排)转向例如,将服务越来越多地“捆绑”在一起,例如,DRGs 和捆绑支付,这种关税表中的不连续性的可能性大大增加。我们的研究说明了这种报销方式的不连续性如何导致提供的医疗保健数量扭曲,从而为关于最佳医疗保健合同设计的辩论做出贡献。