Department of Medicine IV, Medical Center, Faculty of Medicine, University of Freiburg, Freiburg, Germany.
Pharmacy, Medical Center, Faculty of Medicine, University of Freiburg, Freiburg, Germany.
BMC Nephrol. 2023 Aug 10;24(1):235. doi: 10.1186/s12882-023-03288-x.
Primary membranous nephropathy (PMN) frequently causes nephrotic syndrome and declining kidney function. Disease progression is likely modulated by patient-specific and therapy-associated factors awaiting characterization. These cofactors may facilitate identification of risk groups and could result in more individualized therapy recommendations.
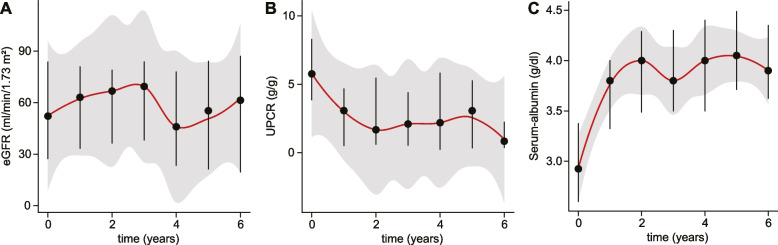
In this single-center retrospective observational study, we analyze the effect of patient-specific and therapy-associated covariates on proteinuria, hypoalbuminemia, and estimated glomerular filtration rate (eGFR) in 74 patients diagnosed with antibody positive PMN and nephrotic-range proteinuria (urine-protein-creatinine-ratio [UPCR] ≥ 3.5 g/g), treated at the University of Freiburg Medical Center between January 2000 - November 2022. The primary endpoint was defined as time to proteinuria / serum-albumin response (UPCR ≤ 0.5 g/g or serum-albumin ≥ 3.5 g/dl), the secondary endpoint as time to permanent eGFR decline (≥ 40% relative to baseline).
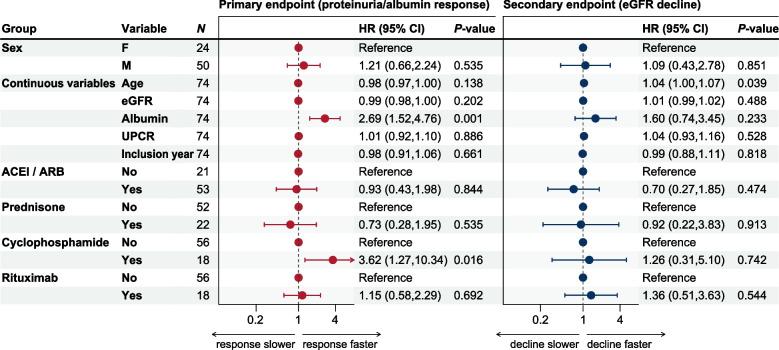
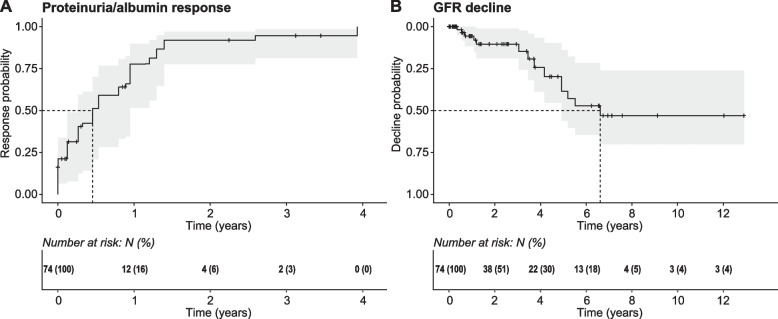
The primary endpoint was reached after 167 days. The secondary endpoint was reached after 2413 days. Multivariate time-to-event analyses showed significantly faster proteinuria / serum-albumin response for higher serum-albumin levels (HR 2.7 [95% CI: 1.5 - 4.8]) and cyclophosphamide treatment (HR 3.6 [95% CI: 1.3 - 10.3]). eGFR decline was significantly faster in subjects with old age at baseline (HR 1.04 [95% CI: 1 - 1.1]).
High serum-albumin levels, and treatment with cyclophosphamide are associated with faster proteinuria reduction and/or serum-albumin normalization. Old age constitutes a risk factor for eGFR decline in subjects with PMN.
原发性膜性肾病(PMN)常导致肾病综合征和肾功能下降。疾病进展可能受到患者特异性和治疗相关因素的调节,这些因素有待进一步明确。这些协变量可能有助于确定风险群体,并可能导致更个体化的治疗建议。
在这项单中心回顾性观察研究中,我们分析了患者特异性和治疗相关协变量对 74 例在弗莱堡大学医学中心诊断为抗体阳性 PMN 伴肾病范围蛋白尿(尿蛋白肌酐比 [UPCR]≥3.5 g/g)的患者的蛋白尿、低白蛋白血症和估算肾小球滤过率(eGFR)的影响,这些患者的治疗时间为 2000 年 1 月至 2022 年 11 月。主要终点定义为蛋白尿/血清白蛋白反应时间(UPCR≤0.5 g/g 或血清白蛋白≥3.5 g/dl),次要终点定义为永久性 eGFR 下降时间(相对于基线下降≥40%)。
主要终点在 167 天后达到。次要终点在 2413 天后达到。多变量生存时间分析显示,血清白蛋白水平较高(HR 2.7 [95% CI:1.5-4.8])和环磷酰胺治疗(HR 3.6 [95% CI:1.3-10.3])与蛋白尿/血清白蛋白反应更快相关。基线时年龄较大的患者 eGFR 下降速度更快(HR 1.04 [95% CI:1-1.1])。
高血清白蛋白水平和环磷酰胺治疗与蛋白尿减少和/或血清白蛋白正常化更快相关。年龄较大是 PMN 患者 eGFR 下降的危险因素。