Fink Christoph A, Weykamp Fabian, Adeberg Sebastian, Bozorgmehr Farastuk, Christopoulos Petros, Lang Kristin, König Laila, Hörner-Rieber Juliane, Thomas Michael, Steins Martin, El-Shafie Rami A, Rieken Stefan, Bernhardt Denise, Debus Jürgen
University Hospital Heidelberg, Department of Radiation Oncology, Heidelberg, Germany.
Heidelberg Institute of Radiation Oncology (HIRO), Germany.
Clin Transl Radiat Oncol. 2023 Jul 24;42:100665. doi: 10.1016/j.ctro.2023.100665. eCollection 2023 Sep.
Combined, platinum-based thoracic chemoradiotherapy (TCR) is the current state-of-the-art treatment for patients with limited disease (LD) small-cell lung cancer (SCLC). There is only limited data available regarding the effect of comorbidities on survival following TRC. The purpose of this study is to assess the age-adjusted Charlson comorbidity index (ACCI) as a predictor of overall survival in LD-SCLC patients undergoing TCR.
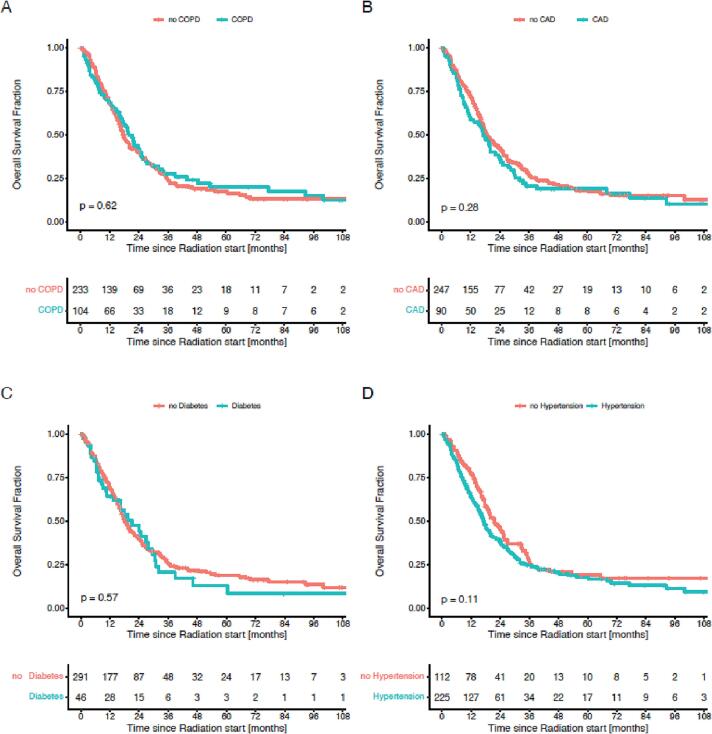
We retrospectively analyzed 367 SCLC patients diagnosed with LD-SCLC who received TCR between 2003 and 2017. We evaluated the ACCI (n = 348) as a predictor of overall survival (OS). In this cohort, 322 patients (88%) received platinum-based TCR (either cisplatin or carboplatin), and 37 (10%) patients received vincristine based TCR. Median radiation dose was 60 Gy (range 24-66 Gy). Additionally, 83% of patients (n = 303) received prophylactic cranial irradiation (PCI, 30 Gy in 2 Gy fractions). Kaplan-Meier survival analysis was performed for OS. For comparison of survival curves, Log-rank (Mantel-Cox) test was used. Univariate and multivariate Cox proportional-hazards ratios (HRs) were used to assess the influence of cofactors on OS.
Patients with an ACCI > 6 had a significantly shorter OS compared with patients with an ACCI ≤ 6 (median 11 vs. 20 months; p = 0.005). Univariate analysis for OS revealed a statistically significant effect for ACCI > 6 (HR 1.7; 95% CI 1.2-2.4; p = 0.003), PCI (HR 0.5; 95% CI 0.3-0.7; p < 0.001), and Karnofsky performance status ≤ 70% (KPS) (HR 1.4; 95% CI 1.1-1.90; p = 0.015). In multivariate analysis, OS was significantly associated with PCI (HR 0.6; 95% CI 0.4-0.9; p = 0.022) and ACCI > 6 (HR 1.5; 95% CI 1.0-2.1; p = 0.049).
Comorbidity is significantly associated with survival in patients with LD-SCLC undergoing TCR. The ACCI may be a valuable tool to identify patients with a shorter survival and thus might be used for risk stratification and oncological decision making.
联合铂类胸段放化疗(TCR)是目前局限期(LD)小细胞肺癌(SCLC)患者的标准治疗方法。关于合并症对TCR后生存影响的数据有限。本研究的目的是评估年龄校正的查尔森合并症指数(ACCI)作为接受TCR的LD-SCLC患者总生存的预测指标。
我们回顾性分析了2003年至2017年间诊断为LD-SCLC并接受TCR的367例SCLC患者。我们评估ACCI(n = 348)作为总生存(OS)的预测指标。在该队列中,322例患者(88%)接受铂类TCR(顺铂或卡铂),37例(10%)患者接受长春新碱为基础的TCR。中位放疗剂量为60 Gy(范围24 - 66 Gy)。此外,83%的患者(n = 303)接受了预防性脑照射(PCI,30 Gy分2 Gy分次)。对OS进行Kaplan-Meier生存分析。为比较生存曲线,采用对数秩(Mantel-Cox)检验。单因素和多因素Cox比例风险比(HR)用于评估协变量对OS的影响。
ACCI > 6的患者与ACCI≤6的患者相比,OS显著缩短(中位时间11个月对20个月;p = 0.005)。OS的单因素分析显示,ACCI > 6(HR 1.7;95%CI 1.2 - 2.4;p = 0.003)、PCI(HR 0.5;95%CI 0.3 - 0.7;p < 0.001)和卡诺夫斯基功能状态≤70%(KPS)(HR 1.4;95%CI 1.1 - 1.90;p = 0.015)有统计学显著影响。在多因素分析中,OS与PCI(HR 0.6;95%CI 0.4 - 0.9;p = 0.022)和ACCI > 6(HR 1.5;95%CI 1.0 - 2.1;p = 0.049)显著相关。
合并症与接受TCR的LD-SCLC患者的生存显著相关。ACCI可能是识别生存较短患者的有价值工具,因此可用于风险分层和肿瘤学决策。