Department of Hepatology, The First Hospital of Jilin University, Jilin Province, China.
Center for Pathogen Biology and Infectious Disease, The First Hospital of Jilin University, Changchun, Jilin Province, China.
Medicine (Baltimore). 2023 Aug 11;102(32):e34291. doi: 10.1097/MD.0000000000034291.
Budd-Chiari Syndrome (BCS) is a relatively rare clinical disorder with a wide range of symptoms, caused by the obstruction of the hepatic venous outflow. The etiology and pathogenesis of BCS vary in different countries and regions. In Western countries, hepatic venous obstruction is the most common type, and its main cause is closely related to the hypercoagulable state of the body. Inferior vena cava obstruction is common in Asia, and its etiology progresses slowly due to the lack of epidemiological data. [3] Here, we report a rare case of BCS associated with the hypereosinophilic syndrome and discuss the possible causal relationship between the two.
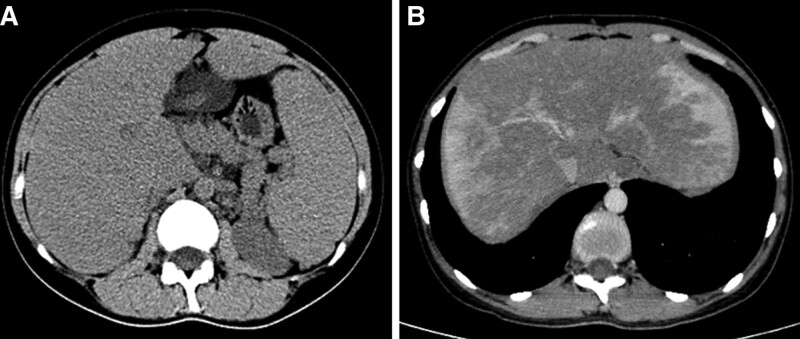
The patient was a 33-year-old female with intermittent epistaxis, gum bleeding, and excessive menstrual flow for the past 6 months. The routine blood tests showed elevated levels of eosinophils, and the liver function test showed mildly elevated levels of γ-glutamyl transpeptidase and alkaline phosphatase, and abdominal ultrasound showed hepatosplenomegaly and suspicion of intrahepatic arteriovenous or arteriovenous-portal fistula.
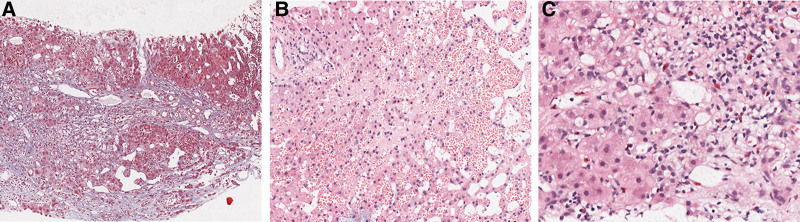
Finally, through the improvement of bone marrow aspiration, digital subtraction angiography and gene detection, the diagnosis of BCS combined with hypereosinophilic syndrome was confirmed, and JAK2V617F mutation was highly associated with it.
The patient received endovascular stent implantation and regular oral rivaroxaban anticoagulation therapy after operation.
Seven months later, enhanced computed tomography (CT) of the hepatobiliary showed that the hepatic bruise-like changes were significantly reduced compared with before, and the right hepatic vein and the right perihepatic vein stent were left in place with a good filling of contrast in the stent.
The patient, in this case, was finally diagnosed with BCS combined with hypereosinophilic syndrome, and to our knowledge, such case reports are rare. Our case report suggest an association between BCS and hypereosinophilic syndrome, but relevant studies are minimal, we hope to conduct larger and higher quality studies on these patients in the future, to provide new directions and basis for the etiology and pathogenesis of these diseases, as well as provide new targets and ideas for clinical treatment.
布加综合征(BCS)是一种相对罕见的临床疾病,其症状多种多样,是由肝静脉流出道阻塞引起的。BCS 的病因和发病机制在不同国家和地区有所不同。在西方国家,肝静脉阻塞是最常见的类型,其主要病因与机体的高凝状态密切相关。下腔静脉阻塞在亚洲较为常见,由于缺乏流行病学数据,其病因进展较为缓慢。[3] 在这里,我们报告了一例与嗜酸性粒细胞增多症相关的 BCS 罕见病例,并探讨了两者之间可能的因果关系。
患者为 33 岁女性,间歇性鼻出血、牙龈出血和月经过多 6 个月。常规血液检查显示嗜酸性粒细胞升高,肝功能检查显示γ-谷氨酰转肽酶和碱性磷酸酶轻度升高,腹部超声显示肝脾肿大,并怀疑肝内动静脉或动静脉-门静脉瘘。
通过骨髓穿刺、数字减影血管造影和基因检测的改善,确诊为 BCS 合并嗜酸性粒细胞增多症,且与 JAK2V617F 突变高度相关。
患者术后接受了血管内支架植入和定期口服利伐沙班抗凝治疗。
7 个月后,肝胆增强 CT 显示肝斑片状改变较前明显减少,右肝静脉及右肝周静脉支架在位,支架内充盈良好。
本例患者最终诊断为 BCS 合并嗜酸性粒细胞增多症,据我们所知,此类病例报告较为罕见。我们的病例报告提示 BCS 与嗜酸性粒细胞增多症之间存在关联,但相关研究较少,我们希望未来能对这些患者进行更大规模和更高质量的研究,为这些疾病的病因和发病机制提供新的方向和依据,并为临床治疗提供新的靶点和思路。