Walsh Jessica A, Saffore Christopher D, Collins Eric B, Ostor Andrew
Division of Rheumatology, Clinic 2, Salt Lake City Veterans Affairs and University of Utah, 50 North Medical Drive, Salt Lake City, UT, 84132, USA.
AbbVie Inc., North Chicago, IL, USA.
Rheumatol Ther. 2023 Oct;10(5):1385-1398. doi: 10.1007/s40744-023-00586-6. Epub 2023 Aug 12.
Recent changes to treatment guidelines for ankylosing spondylitis (AS) have listed first-line advanced therapies as tumor necrosis factor (TNF), interleukin (IL)-17, and Janus kinase (JAK) inhibitors. This study sought to assess the comparative clinical and economic benefit of advanced therapies approved for AS.
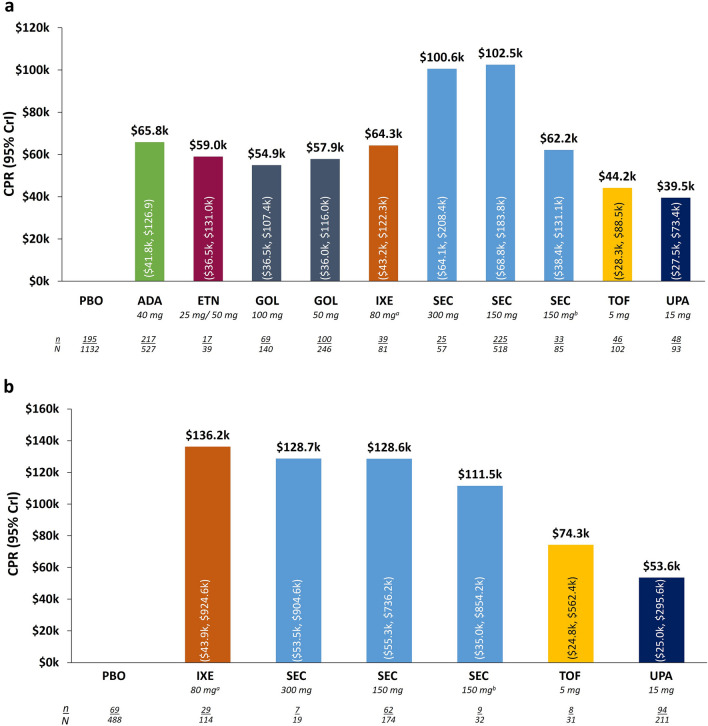
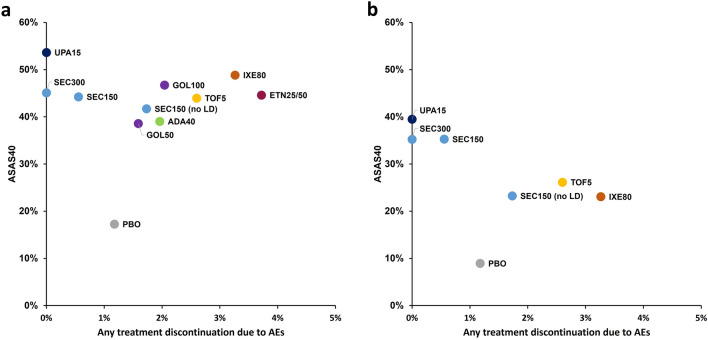
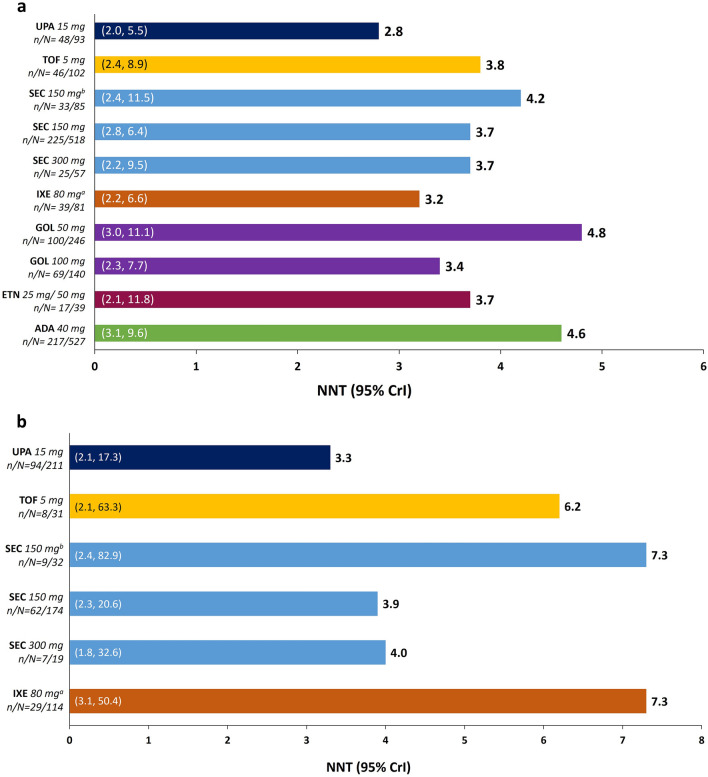
A systematic literature review was conducted to identify randomized clinical trials for JAK inhibitors (upadacitinib [UPA], tofacitinib [TOF]), anti-IL-17 therapies (secukinumab [SEC], ixekizumab [IXE]), and TNF inhibitors (adalimumab [ADA], etanercept [ETN], golimumab [GOL]) used for the treatment of active AS. Clinical efficacy was evaluated by Assessment of Spondyloarthritis International Society 40 (ASAS40) criteria and treatment discontinuation due to adverse events (AEs) was used to generate response rates synthesized via a Bayesian network meta-analysis. Number needed to treat (NNT) was calculated as the reciprocal of incremental response rate of each treatment versus placebo. Cost per ASAS40 responder (CPR) was calculated as the 12-week treatment costs divided by ASAS40 response rates. Data were stratified by biologic treatment status (i.e., biologic naïve [bio-naïve] or inadequate response or intolerance to biologics [bio-IR]) for efficacy and CPR analyses.
Among bio-naïve patients, the response rate for ASAS40 was 53.6% for UPA-treated patients, whereas most other treatments had response rates between 41% and 49%. NNTs were lowest for UPA-treated patients at 2.8 (other therapies 3.2-4.8). Estimated CPR among UPA-treated patients was lowest (UPA $39.5k vs others $44.2k-102.5k). Efficacy and CPR trends were similar among bio-IR and TNF-IR patients. Among bio-naïve and bio-IR patients, the rate of AEs leading to discontinuation was lowest among UPA and SEC-treated patients (0.0, others 0.6-3.7%).
Relative to other treatments assessed in this study, UPA demonstrated numerically greater clinical and economic benefit for the treatment of AS. Head-to-head or real-world comparisons of these therapies are warranted and may inform clinical decision-making.
强直性脊柱炎(AS)治疗指南最近的变化将一线先进疗法列为肿瘤坏死因子(TNF)、白细胞介素(IL)-17和Janus激酶(JAK)抑制剂。本研究旨在评估批准用于AS的先进疗法的临床和经济效益比较。
进行系统的文献综述,以确定用于治疗活动性AS的JAK抑制剂(乌帕替尼[UPA]、托法替布[TOF])、抗IL-17疗法(司库奇尤单抗[SEC]、依奇珠单抗[IXE])和TNF抑制剂(阿达木单抗[ADA]、依那西普[ETN]、戈利木单抗[GOL])的随机临床试验。通过国际脊柱关节炎评估协会40(ASAS40)标准评估临床疗效,并使用因不良事件(AE)导致的治疗中断来生成通过贝叶斯网络荟萃分析合成的缓解率。治疗所需人数(NNT)计算为每种治疗与安慰剂相比的增量缓解率的倒数。每例ASAS40缓解者的成本(CPR)计算为12周治疗成本除以ASAS40缓解率。数据按生物治疗状态(即初治生物制剂[生物初治]或对生物制剂反应不足或不耐受[生物制剂反应不佳])分层进行疗效和CPR分析。
在生物初治患者中,UPA治疗患者的ASAS40缓解率为53.6%,而大多数其他治疗的缓解率在41%至49%之间。UPA治疗患者的NNT最低,为2.8(其他疗法为3.2 - 4.8)。UPA治疗患者的估计CPR最低(UPA为39.5k美元,其他为44.2k - 102.5k美元)。生物制剂反应不佳和TNF反应不佳患者的疗效和CPR趋势相似。在生物初治和生物制剂反应不佳患者中,UPA和SEC治疗患者因AE导致停药的发生率最低(0.0,其他为0.6 - 3.7%)。
相对于本研究中评估的其他治疗,UPA在治疗AS方面显示出更大的临床和经济效益。有必要对这些疗法进行头对头或真实世界的比较,这可能为临床决策提供参考。