Bock Matthias, O'Connor Matthew, Chouchane Amir, Schmidt Philip, Schaarschmidt Claudia, Knoll Katharina, Bahlke Fabian, Englert Florian, Storz Theresa, Kottmaier Marc, Trenkwalder Teresa, Reents Tilko, Bourier Felix, Telishevska Marta, Lengauer Sarah, Hessling Gabriele, Deisenhofer Isabel, Kolb Christof, Lennerz Carsten
German Heart Centre Munich, Department of Electrophysiology, Technical University of Munich, 80636 Munich, Germany.
DZHK (German Centre for Cardiovascular Research, Partner Site Munich, Heart Alliance), 80336 Munich, Germany.
J Clin Med. 2023 Jul 26;12(15):4900. doi: 10.3390/jcm12154900.
The demand for transvenous lead extraction (TLE) has increased. In line with this, the safety of such procedures has also increased. Traditionally, TLE is performed under resource-intensive general anaesthesia. This study aims to evaluate the safety and outcomes of Cardiologist-lead deep sedation for TLE.
We retrospectively analysed 328 TLE procedures performed under deep sedation from 2016 to 2019. TLE procedures were performed by experienced electrophysiologists. Sedation was administered by a specifically trained cardiologist (bolus midazolam/fentanyl and propofol infusion). Procedural sedation data including blood pressure, medication administration and sedation time were collected. Complications related to sedation and the operative component of the procedure were analysed retrospectively.
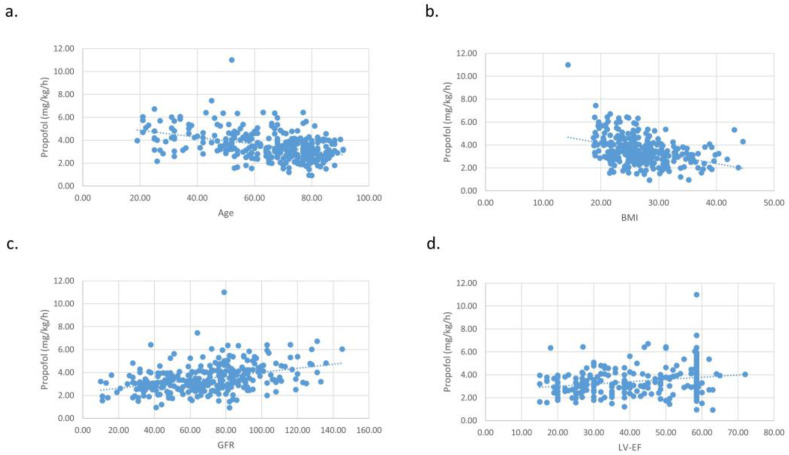
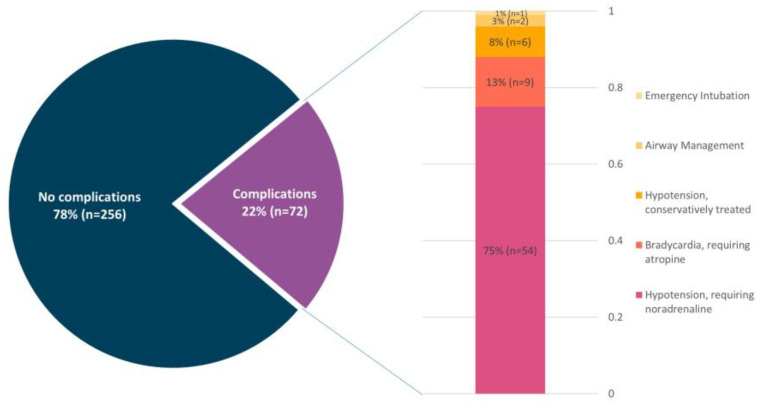
The sedation-associated complication rate during TLE was 22.0%. The most common complication (75% of complications) was hypotension requiring noradrenaline, followed by bradycardia requiring atropine (13% of complications). Additionally, the unplanned presence of an anaesthesiologist was needed in one case (0.3%). Deep sedation was achieved with midazolam (mean dose 42.9 ± 26.5 µg/kg), fentanyl (mean dose 0.4 ± 0.6 µg/kg) and propofol (mean dose 3.5 ± 1.2 mg/kg/h). There was no difference in medication dosage between those with a sedation-associated complication and those without. Sedation-associated complications appeared significantly more in patients with reduced LVEF ( = 0.01), renal impairment ( = 0.01) and a higher American Society of Anaesthesiologists (ASA) class ( = 0.01).
Deep sedation for TLE can be safely performed by a specifically trained cardiologist, with a transition to general anaesthesia required in only 0.3% of cases. We continue to recommend the on-call availability of an anaesthesiologist and cardiac surgeon in case of major complications.
经静脉导线拔除术(TLE)的需求有所增加。与此相应,此类手术的安全性也有所提高。传统上,TLE是在资源密集型的全身麻醉下进行的。本研究旨在评估由心脏病专家主导的深度镇静用于TLE的安全性和结果。
我们回顾性分析了2016年至2019年在深度镇静下进行的328例TLE手术。TLE手术由经验丰富的电生理学家进行。镇静由经过专门培训的心脏病专家实施(静脉推注咪达唑仑/芬太尼和输注丙泊酚)。收集包括血压、药物给药和镇静时间在内的手术镇静数据。回顾性分析与镇静及手术操作相关的并发症。
TLE期间与镇静相关的并发症发生率为22.0%。最常见的并发症(占并发症的75%)是需要去甲肾上腺素治疗的低血压,其次是需要阿托品治疗的心动过缓(占并发症的13%)。此外,有1例(0.3%)需要麻醉医生意外到场。使用咪达唑仑(平均剂量42.9±26.5μg/kg)、芬太尼(平均剂量0.4±0.6μg/kg)和丙泊酚(平均剂量3.5±1.2mg/kg/h)实现了深度镇静。发生与镇静相关并发症的患者和未发生并发症的患者之间药物剂量没有差异。左心室射血分数降低(P = 0.01)、肾功能损害(P = 0.01)和美国麻醉医师协会(ASA)分级较高(P = 0.01)的患者中,与镇静相关的并发症明显更多。
经过专门培训的心脏病专家可以安全地对TLE实施深度镇静,仅0.3%的病例需要转为全身麻醉。我们继续建议在出现重大并发症时麻醉医生和心脏外科医生随时待命。