Shenzhen Campus of Sun Yat-sen University, No. 66, Gongchang Road, Guangming District, Shenzhen, 518107, Guangdong, People's Republic of China.
School of Public Health (Shenzhen), Sun Yat-sen University, No. 66, Gongchang Road, Guangming District, Shenzhen, 518107, Guangdong, People's Republic of China.
Infect Dis Poverty. 2023 Aug 14;12(1):73. doi: 10.1186/s40249-023-01119-7.
In 2003, China implemented free antiretroviral therapy (ART) for people living with HIV (PLHIV), establishing an eligibility threshold of CD4 < 200 cells/μl. Subsequently, the entry criteria were revised in 2012 (eligibility threshold: CD4 ≤ 350 cells/μl), 2014 (CD4 ≤ 500 cells/μl), and 2016 (treat-all). However, the impact of treat-all policy on HIV care and treatment indicators in China is unknown. We aimed to elucidate the immediate and long-term impact of the implementation of treat-all policy in China.
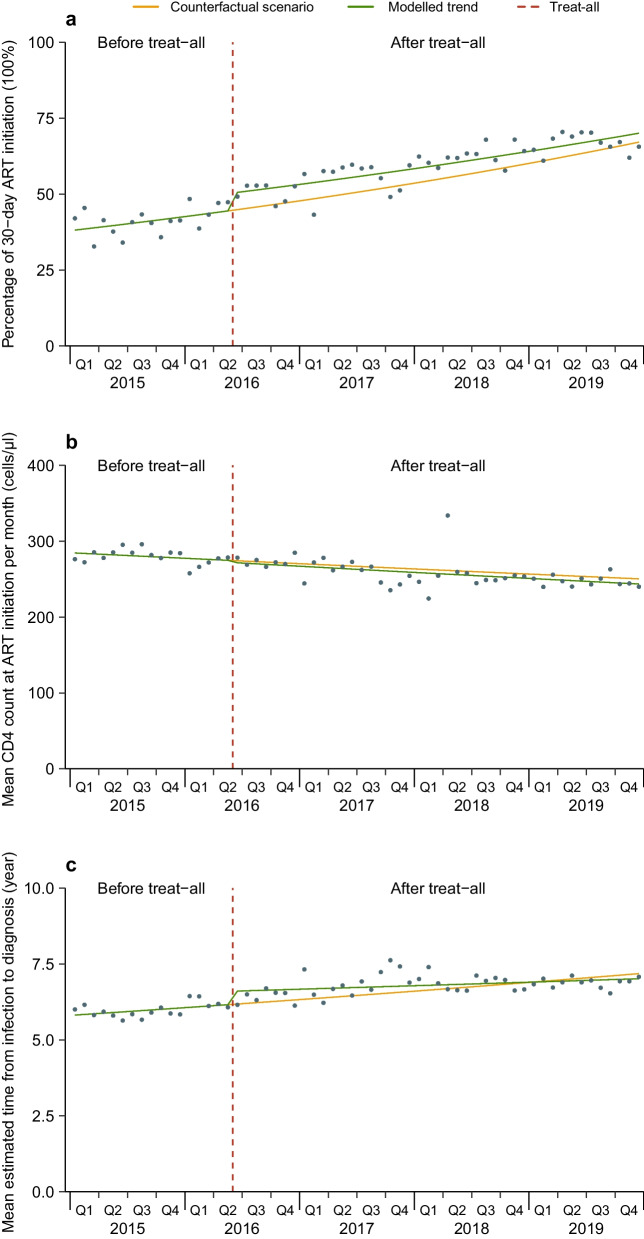
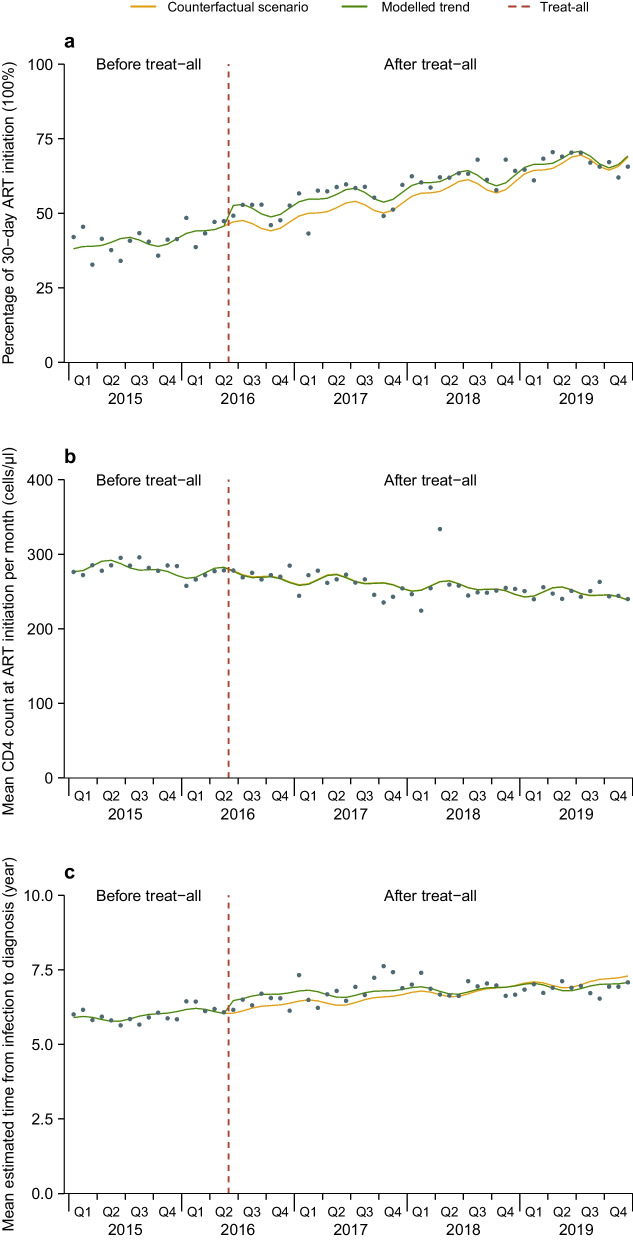
Anonymized programmatic data on ART initiation and collection in PLHIV who newly started ART were retrieved between 1 January 2015 and 31 December 2019, from two provincial and municipal Centers for Disease Control and Prevention and ten major infectious disease hospitals specialized in HIV care in China. We used Poisson and quasi-Poisson segmented regression models to estimate the immediate and long-term impact of treat-all on three key indicators: monthly proportion of 30-day ART initiation, mean CD4 counts (cells/μl) at ART initiation, and mean estimated time from infection to diagnosis (year). We built separate models according to gender, age, route of transmission and region.
Monthly data on ART initiation and collection were available for 75,516 individuals [gender: 83.8% males; age: median 39 years, interquartile range (IQR): 28-53; region: 18.5% Northern China, 10.9% Northeastern China, 17.5% Southern China, 49.2% Southwestern China]. In the first month of treat-all, compared with the contemporaneous counterfactual, there was a significant increase in proportion of 30-day ART initiation [+ 12.6%, incidence rate ratio (IRR) = 1.126, 95% CI: 1.033-1.229; P = 0.007] and mean estimated time from infection to diagnosis (+ 7.0%, IRR = 1.070, 95% CI: 1.021-1.120; P = 0.004), while there was no significant change in mean CD4 at ART initiation (IRR = 0.990, 95% CI: 0.956-1.026; P = 0.585). By December 2019, the three outcomes were not significantly different from expected levels. In the stratified analysis, compared with the contemporaneous counterfactual, mean CD4 at ART initiation showed significant increases in Northern China (+ 3.3%, IRR = 1.033, 95% CI: 1.001-1.065; P = 0.041) and Northeastern China (+ 8.0%, IRR = 1.080, 95% CI: 1.003-1.164; P = 0.042) in the first month of treat-all; mean estimated time from infection to diagnosis showed significant increases in male (+ 5.6%, IRR = 1.056, 95% CI: 1.010-1.104; P = 0.016), female (+ 14.8%, IRR = 1.148, 95% CI: 1.062-1.240; P < 0.001), aged 26-35 (+ 5.3%, IRR = 1.053, 95% CI: 1.001-1.109; P = 0.048) and > 50 (+ 7.8%, IRR = 1.078, 95% CI: 1.000-1.161; P = 0.046), heterosexual transmission (+ 12.4%, IRR = 1.124, 95% CI: 1.042-1.213; P = 0.002) and Southwestern China (+ 12.9%, IRR = 1.129, 95% CI: 1.055-1.208; P < 0.001) in the first month of treat-all.
The implementation of treat-all policy in China was associated with a positive effect on HIV care and treatment outcomes. To advance the work of rapid ART, efforts should be made to streamline the testing and ART initiation process, provide comprehensive support services, and address the issue of uneven distribution of medical resources.
2003 年,中国开始为艾滋病毒感染者(PLHIV)提供免费抗逆转录病毒治疗(ART),并设定了 CD4<200 个细胞/μl 的准入门槛。随后,准入标准分别于 2012 年(准入标准:CD4≤350 个细胞/μl)、2014 年(CD4≤500 个细胞/μl)和 2016 年(全面治疗)进行了修订。然而,在中国实施全面治疗政策对艾滋病毒护理和治疗指标的影响尚不清楚。我们旨在阐明中国实施全面治疗政策的即时和长期影响。
我们从中国两个省级和市级疾病预防控制中心以及十家专门从事艾滋病毒护理的主要传染病医院,检索了 2015 年 1 月 1 日至 2019 年 12 月 31 日期间新开始接受 ART 的 PLHIV 的 ART 启动和收集的匿名项目数据。我们使用泊松和拟泊松分段回归模型来估计全面治疗对三个关键指标的即时和长期影响:30 天内开始 ART 的月度比例、开始 ART 时的平均 CD4 计数(细胞/μl)和从感染到诊断的平均估计时间(年)。我们根据性别、年龄、传播途径和地区分别建立了模型。
我们获得了 75516 名个体的 ART 启动和收集月度数据[性别:83.8%为男性;年龄:中位数为 39 岁,四分位间距(IQR)为 28-53;地区:18.5%为中国北方,10.9%为中国东北,17.5%为中国南方,49.2%为中国西南]。在全面治疗的第一个月,与同期的对照情况相比,30 天内开始 ART 的比例显著增加[+12.6%,发病率比(IRR)=1.126,95%置信区间(CI):1.033-1.229;P=0.007],从感染到诊断的平均估计时间也有所增加(+7.0%,IRR=1.070,95%CI:1.021-1.120;P=0.004),而开始 ART 时的平均 CD4 计数没有显著变化(IRR=0.990,95%CI:0.956-1.026;P=0.585)。到 2019 年 12 月,这三个结果与预期水平没有显著差异。在分层分析中,与同期的对照情况相比,中国北方和中国东北的开始 ART 时的平均 CD4 计数在全面治疗的第一个月显示出显著增加[中国北方:+3.3%,IRR=1.033,95%CI:1.001-1.065;P=0.041;中国东北:+8.0%,IRR=1.080,95%CI:1.003-1.164;P=0.042];从感染到诊断的平均估计时间在全面治疗的第一个月也显示出显著增加[男性:+5.6%,IRR=1.056,95%CI:1.010-1.104;P=0.016;女性:+14.8%,IRR=1.148,95%CI:1.062-1.240;P<0.001;年龄 26-35 岁:+5.3%,IRR=1.053,95%CI:1.001-1.109;P=0.048;>50 岁:+7.8%,IRR=1.078,95%CI:1.000-1.161;P=0.046];异性传播:+12.4%,IRR=1.124,95%CI:1.042-1.213;P=0.002]和中国西南地区:+12.9%,IRR=1.129,95%CI:1.055-1.208;P<0.001)。
中国实施全面治疗政策与艾滋病毒护理和治疗结果的积极影响相关。为了推进快速 ART 工作,应努力简化检测和 ART 启动流程,提供全面的支持服务,并解决医疗资源分布不均的问题。