Gwacham-Anisiobi Uchenna, Boo Yebeen Ysabelle, Oladimeji Adetola, Kurinczuk Jennifer J, Roberts Nia, Opondo Charles, Nair Manisha
National Perinatal Epidemiology Unit, Nuffield Department of Population Health, University of Oxford, Oxford, United Kingdom.
Solina Center for International Development and Research, Nigeria.
EClinicalMedicine. 2023 Aug 3;62:102133. doi: 10.1016/j.eclinm.2023.102133. eCollection 2023 Aug.
Community-based interventions are increasingly being implemented in Sub-Saharan Africa (SSA) for stillbirth prevention, but the nature of these interventions, their reporting and acceptability are poorly assessed. In addition to understanding their effectiveness, complete reporting of the methods, results and intervention acceptability is essential as it could potentially reduce research waste from replication of inadequately implemented and unacceptable interventions. We conducted a systematic review to investigate these aspects of community-based interventions for preventing stillbirths in SSA.
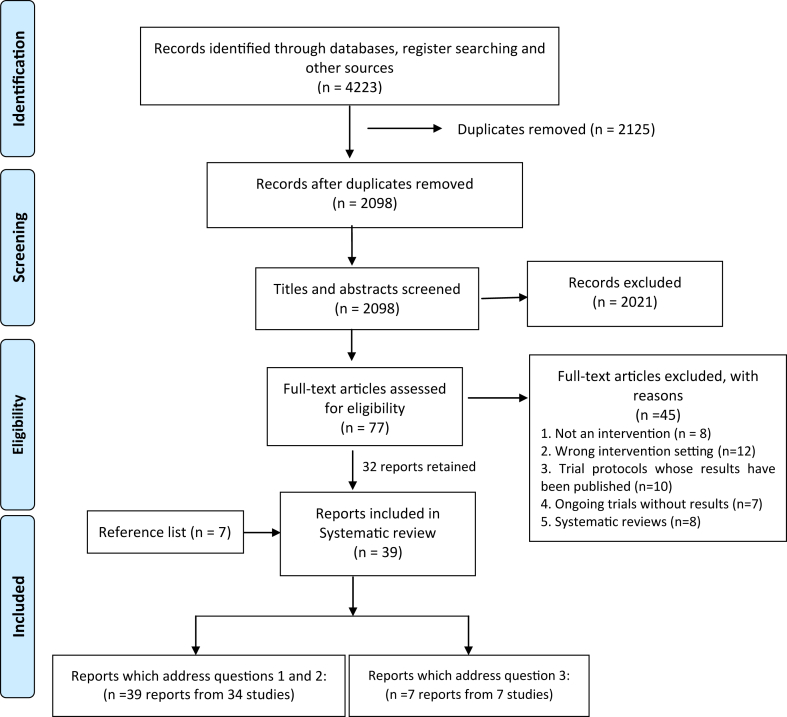
In this systematic review, eight databases (MEDLINE(OvidSP), Embase (OvidSP), Cochrane Central Register of Controlled Trials, Global Health, Science Citation Index and Social Science Citation index (Web of Science Core Collection), CINAHL (EBSCOhost) and Global Index Medicus) and four grey literature sources were searched from January 1, 2000 to July 7, 2023 for relevant quantitative and qualitative studies from SSA (PROSPERO-CRD42021296623). Following deduplication, abstract screening and full-text review, studies were included if the interventions were community-based with or without a health facility component. The main outcomes were types of community-based interventions, completeness of intervention reporting using the TIDier (Template for Intervention Description and replication) checklist, and themes related to intervention acceptability identified using a theoretical framework. Study quality was assessed using the Cochrane risk of bias and National Heart, Lung and Blood Institute's tools.
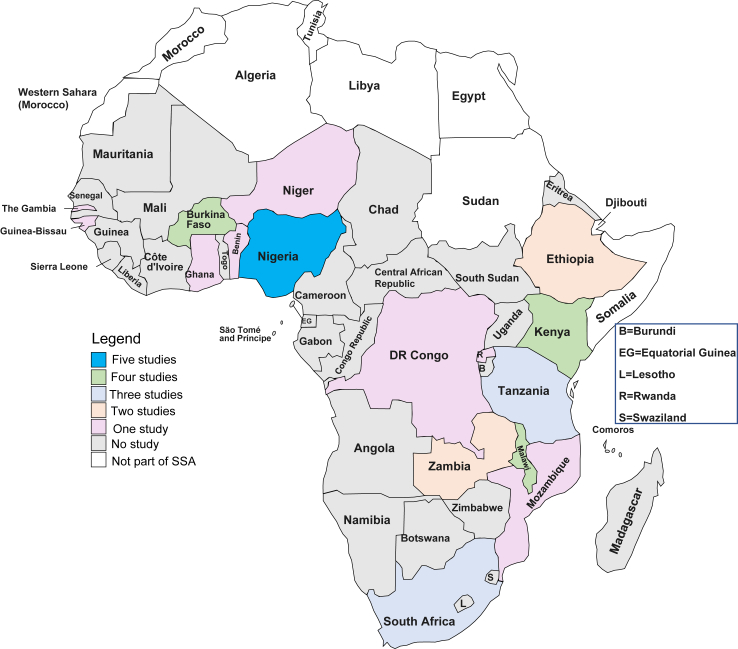
Thirty-nine reports from thirty-four studies conducted in 18 SSA countries were eligible for inclusion. Four types of interventions were identified: nutritional, infection prevention, access to skilled childbirth attendants and health knowledge/behaviour of women. These interventions were implemented using nine strategies: mHealth (defined as the use of mobile and wireless technologies to support the achievement of health objectives), women's groups, community midwifery, home visits, mass media sensitisation, traditional birth attendant and community volunteer training, community mobilisation and transport vouchers. The completeness of reporting using the TIDier checklist varied across studies with a very low proportion of the included studies reporting the intervention intensity, dosing, tailoring and modification. The quality of the included studies were graded as poor (n = 6), fair (n = 14) and good (n = 18). Though interventions were acceptable, only 4 (out of 7) studies explored women's perceptions, mostly focusing on perceived intervention effects and how they felt, omitting key constructs like ethicality, opportunity cost and burden of participation.
Different community-based interventions have been tried and evaluated for stillbirth prevention in SSA. The reproducibility and implementation scale-up of these interventions may be limited by incomplete intervention descriptions in the published literature. To strengthen impact, it is crucial to holistically explore the acceptability of these interventions among women and their families.
Clarendon/Balliol/NDPH DPhil scholarship for UGA. MN is funded by a Medical Research Council Transition Support Award (MR/W029294/1).
撒哈拉以南非洲地区(SSA)越来越多地实施基于社区的干预措施来预防死产,但这些干预措施的性质、报告情况和可接受性评估不足。除了了解其有效性外,完整报告方法、结果和干预措施的可接受性至关重要,因为这可能会减少因重复实施不充分和不可接受的干预措施而造成的研究浪费。我们进行了一项系统综述,以调查SSA地区基于社区的死产预防干预措施的这些方面。
在这项系统综述中,检索了八个数据库(MEDLINE(OvidSP)、Embase(OvidSP)、Cochrane对照试验中央注册库、全球卫生、科学引文索引和社会科学引文索引(Web of Science核心合集)、CINAHL(EBSCOhost)和全球医学索引)以及四个灰色文献来源,以查找2000年1月1日至2023年7月7日期间来自SSA的相关定量和定性研究(PROSPERO-CRD42021296623)。在进行重复数据删除、摘要筛选和全文审查后,如果干预措施是以社区为基础的,无论是否包含卫生设施部分,则纳入研究。主要结果包括基于社区的干预措施类型、使用TIDier(干预描述和复制模板)清单的干预报告完整性,以及使用理论框架确定的与干预可接受性相关的主题。使用Cochrane偏倚风险工具和美国国立心肺血液研究所的工具评估研究质量。
在18个SSA国家进行的34项研究中的39份报告符合纳入条件。确定了四种干预类型:营养、感染预防、获得熟练的分娩护理人员以及妇女的健康知识/行为。这些干预措施通过九种策略实施:移动健康(定义为使用移动和无线技术支持实现健康目标)、妇女团体、社区助产、家访、大众媒体宣传、传统助产士和社区志愿者培训、社区动员和交通券。使用TIDier清单的报告完整性在不同研究中有所不同,纳入研究中报告干预强度、剂量、定制和修改的比例非常低。纳入研究的质量分为差(n = 6)、一般(n = 14)和好(n = 18)。尽管干预措施是可接受的,但只有4项(共7项)研究探讨了妇女的看法,主要关注感知到的干预效果以及她们的感受,遗漏了诸如道德性、机会成本和参与负担等关键因素。
在SSA地区,已经尝试并评估了不同的基于社区的死产预防干预措施。这些干预措施的可重复性和实施推广可能受到已发表文献中干预描述不完整的限制。为了加强影响,全面探索这些干预措施在妇女及其家庭中的可接受性至关重要。
为UGA提供的克拉伦登/贝利奥尔学院/ NDPH哲学博士奖学金。MN由医学研究理事会过渡支持奖(MR/W029294/1)资助。