Institute of Cardiovascular Science, University College London, United Kingdom (D.E.C., A.P., A.B., P.S., M.L., P.M.E.).
Department of Inherited Cardiovascular Diseases, Barts Heart Centre, St Bartholomew's Hospital, London, United Kingdom (D.E.C., A.P., A.B., M.L., P.M.E.).
Circ Genom Precis Med. 2023 Oct;16(5):434-441. doi: 10.1161/CIRCGEN.123.004059. Epub 2023 Aug 18.
Variants in are reported in 2% to 6% of familial cases of dilated cardiomyopathy and may be associated with fatal ventricular arrhythmia and rapid heart failure progression. We sought to determine the risk of adverse events in variant carriers and the impact of sex on outcomes.
Consecutive probands and relatives carrying variants were retrospectively recruited from 12 cardiomyopathy units. The primary end point was a composite of malignant ventricular arrhythmia (MVA) and end-stage heart failure (ESHF). MVA and ESHF end points were also analyzed separately and men and women compared. Left ventricular ejection fraction (LVEF) contemporary to MVA was examined. variant carriers with left ventricular systolic dysfunction () were compared with variant-elusive patients with idiopathic left ventricular systolic dysfunction.
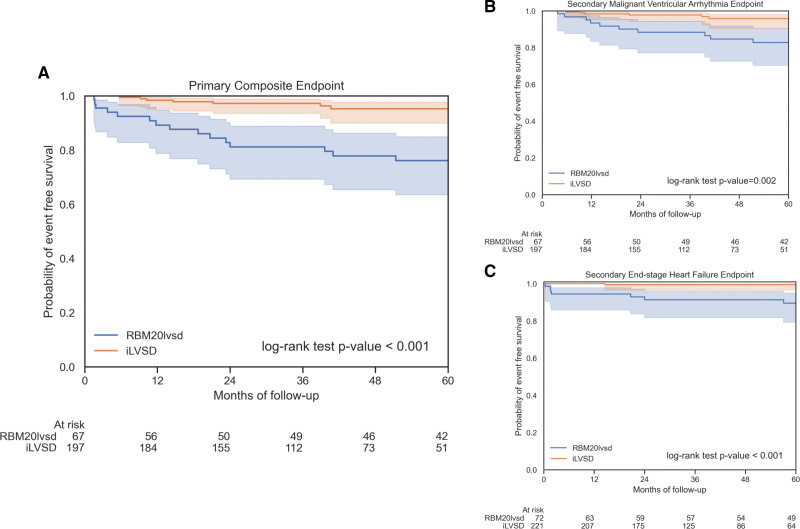
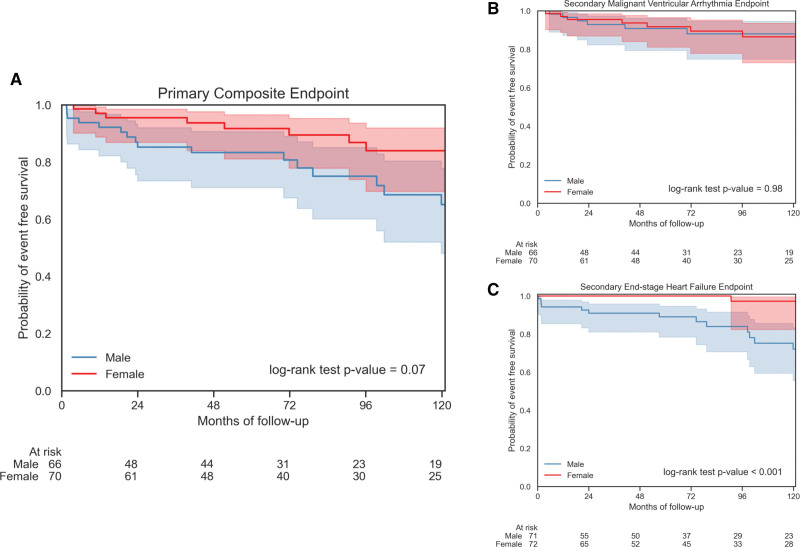
Longitudinal follow-up data were available for 143 variant carriers (71 men; median age, 35.5 years); 7 of 143 had an MVA event at baseline. Thirty of 136 without baseline MVA (22.0%) reached the primary end point, and 16 of 136 (11.8%) had new MVA with no significant difference between men and women (log-rank =0.07 and =0.98, respectively). Twenty of 143 (14.0%) developed ESHF (17 men and 3 women; log-rank <0.001). Four of 10 variant carriers with available LVEF contemporary to MVA had an LVEF >35%. At 5 years, 15 of 67 (22.4%) versus 7 of 197 (3.6%) patients with idiopathic left ventricular systolic dysfunction had reached the primary end point (log-rank <0.001). variant carriage conferred a 6.0-fold increase in risk of the primary end point.
variants are associated with a high risk of MVA and ESHF compared with idiopathic left ventricular systolic dysfunction. The risk of MVA in male and female variant carriers is similar, but male sex is strongly associated with ESHF.
在 2%至 6%的扩张型心肌病家族病例中发现了 基因的变异,这些变异可能与致命性室性心律失常和快速心力衰竭进展有关。我们试图确定 变异携带者发生不良事件的风险,以及性别对结果的影响。
连续从 12 个心肌病单位招募携带 基因变异的先证者及其亲属。主要终点是恶性室性心律失常(MVA)和终末期心力衰竭(ESHF)的复合终点。还分别分析了 MVA 和 ESHF 终点,并对男性和女性进行了比较。同时还检查了 MVA 时的左心室射血分数(LVEF)。与特发性左心室收缩功能障碍的 变异逃避患者相比,伴有左心室收缩功能障碍()的 变异携带者也进行了比较。
143 名 变异携带者(71 名男性;中位年龄 35.5 岁)有纵向随访数据;其中 143 名中有 7 名在基线时发生 MVA 事件。136 名无基线 MVA 的患者中,30 名(22.0%)达到主要终点,136 名中有 16 名(11.8%)出现新的 MVA,男性和女性之间无显著差异(对数秩=0.07,=0.98)。143 名患者中有 20 名(14.0%)发生 ESHF(17 名男性和 3 名女性;对数秩<0.001)。在有 MVA 时可获得 LVEF 的 10 名 变异携带者中,有 4 名的 LVEF>35%。在 5 年时,67 名患者中有 15 名(22.4%)达到了主要终点,而 197 名特发性左心室收缩功能障碍患者中有 7 名(3.6%)达到了主要终点(对数秩<0.001)。携带 变异使发生主要终点的风险增加了 6.0 倍。
与特发性左心室收缩功能障碍相比, 基因变异与恶性室性心律失常和终末期心力衰竭的风险增加相关。男性和女性 变异携带者的 MVA 风险相似,但男性与 ESHF 强烈相关。